Non-accidental head trauma/ Abusive head trauma
Title: Non-accidental head trauma/Abusive head trauma
Authors: Alvina Liang, BS; Theresa Long, MD
Photographer: Lisa Messegee
Date: 7/6/2025
Keywords/Main Subjects: Non-Accidental Head Trauma
Diagnosis: Non-accidental head trauma (Shaken Baby Syndrome)
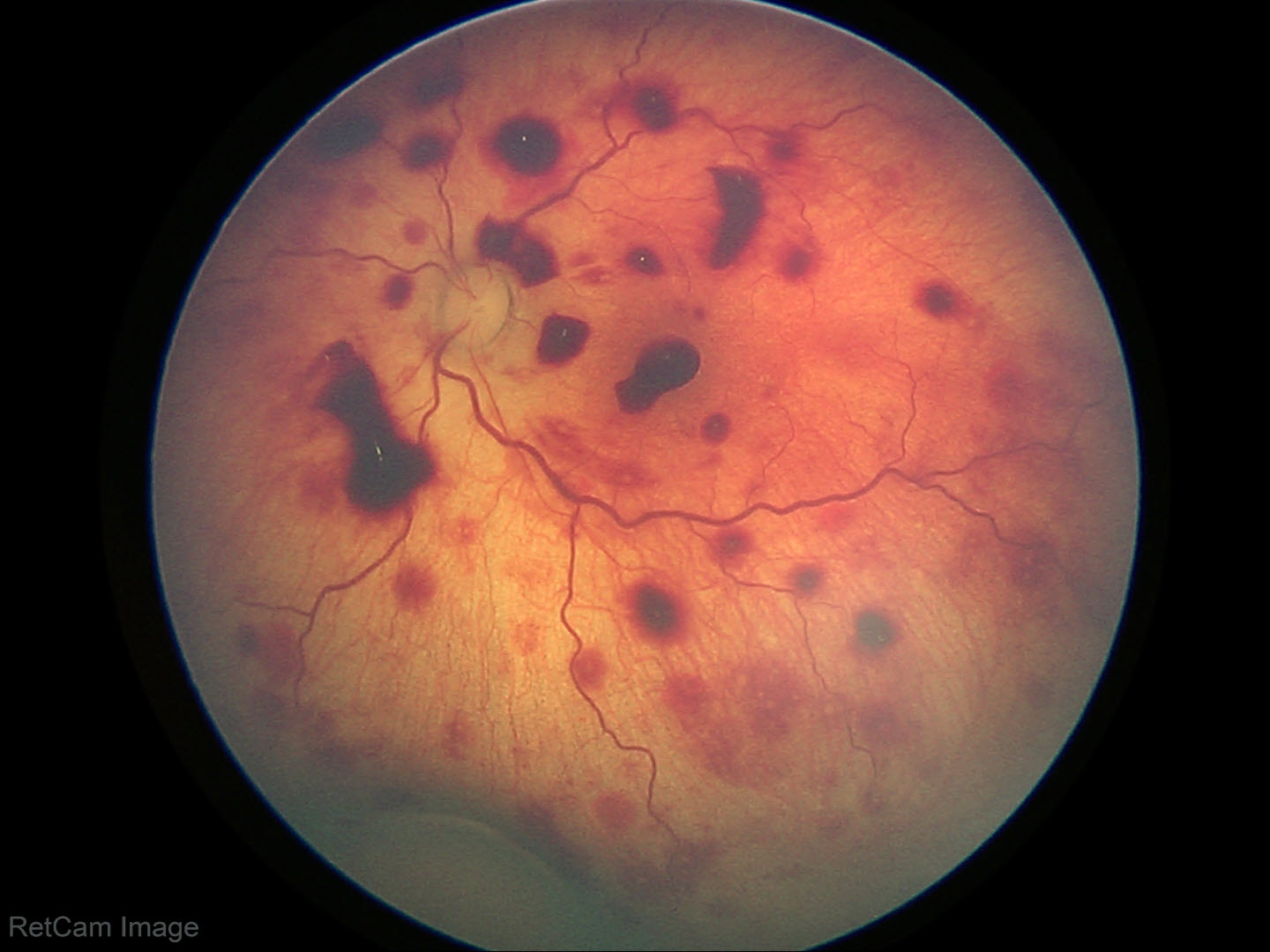
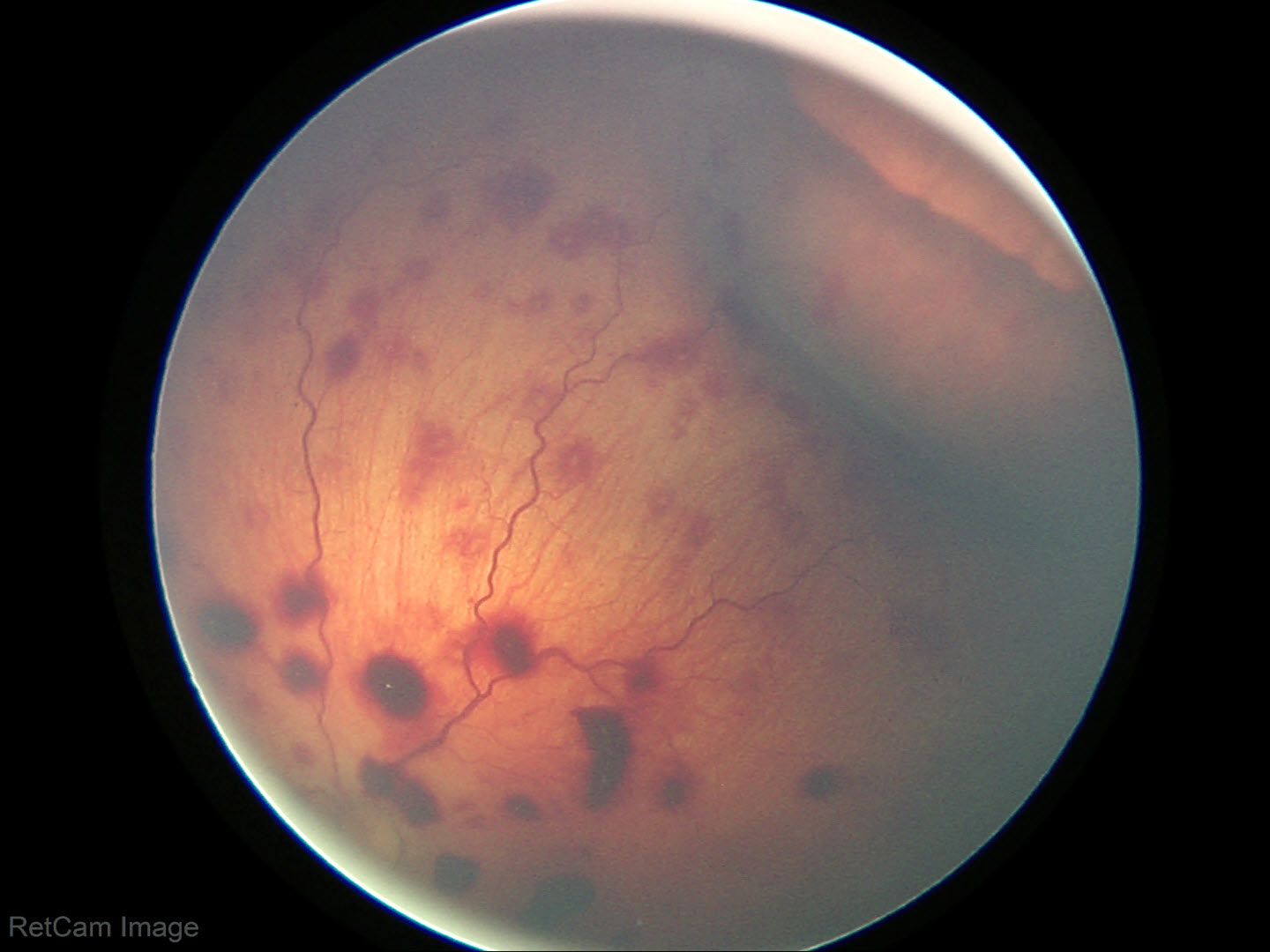
Description of Image:
Extensive preretinal, subretinal and intraretinal hemorrhages in all retinal quadrants. (Blot hemorrhages, flame hemorrhages, white centered hemorrhages). Tortuous vessels.
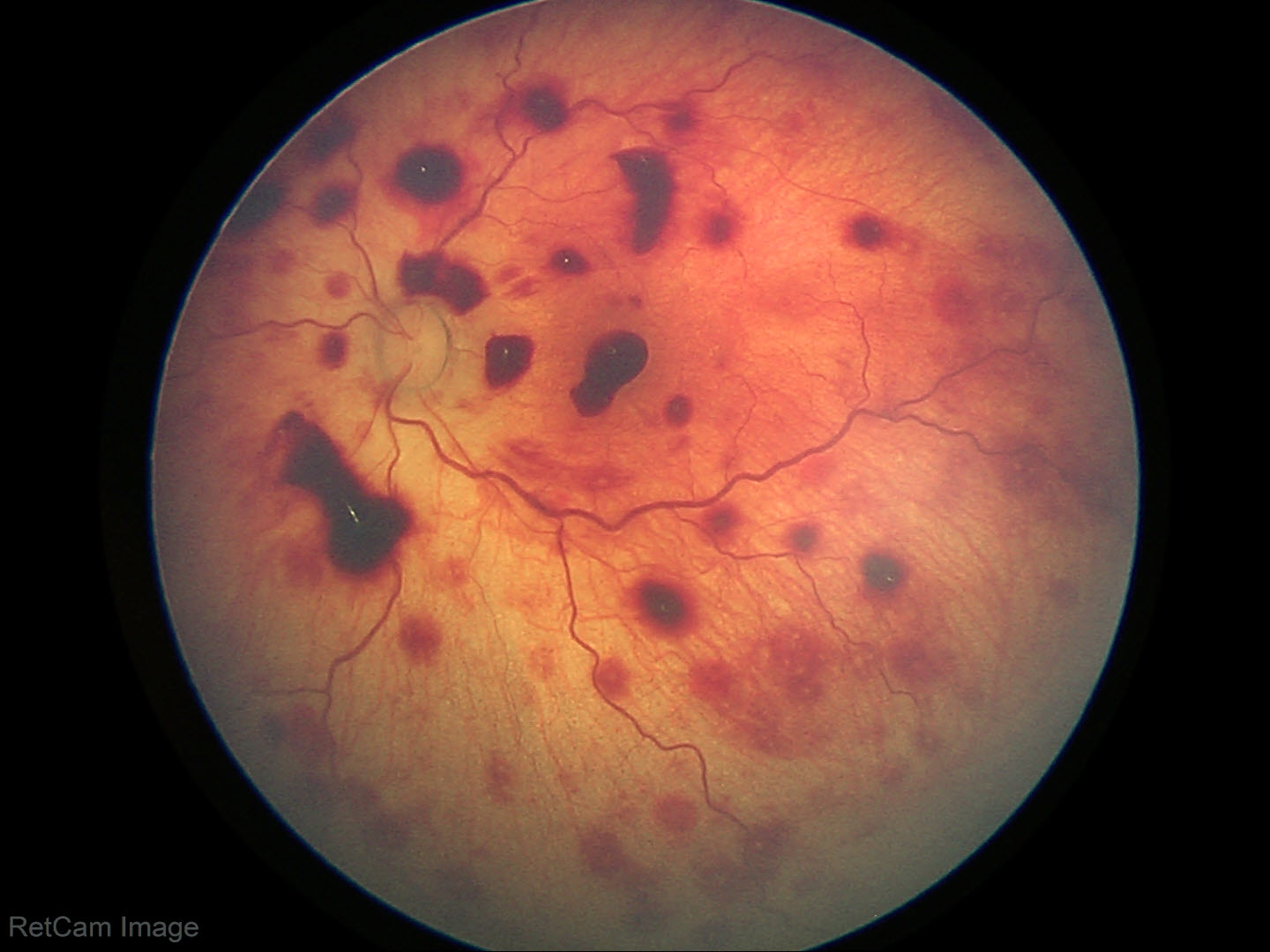
Extensive retinal hemorrhages, extending to the ora serrata on scleral depressed examination.
Introduction
Pediatric abusive head trauma (AHT), also known as shaken baby syndrome (SBS), is a form of child abuse that is defined as “an injury to the skull or intracranial contents of an infant or young child (<5 years of age) due to inflicted blunt impact and/or violent shaking.1,2
Epidemiology
AHT is the third leading cause of head injury in children younger than 5 years, following motor vehicle collision and falls,3 with a reported incidence of between 22 to 40 per 100,000 children3,4 and a mortality rate between 10-20%. 4,5
Common Findings
Physical and radiological imaging findings of AHT are results of primary and secondary injuries. The primary injuries, consequences of the initial direct trauma or impact, can include skull fracture, cortical contusion, diffuse axonal injury, epidural, subdural, subarachnoid, and intraparenchymal hemorrhages.6 Secondary injuries are results from complications of the primary injury and involve biomolecular inflammatory changes of the brain.7 These can include diffuse brain edema, herniation, infarction or cerebrovascular accidents.6
Ocular findings
It is estimated that around 5% of AHT cases present with ocular findings. Ocular findings of AHT most often include retinal hemorrhages, including intraretinal, subretinal, preretinal hemorrhages, seen in 85% of cases.8 Vitreous hemorrhages, macular retinoschisis, retinal tears, retinal detachments have also been reported.9 The presence of circumferential perimacularretinal folds,10 optic disc hemorrhages, papilledema, and optic disc pallor and atrophy has also been associated with AHT.
While retinal hemorrhages are not pathognomonic for abusive head trauma, they are strongly associated with it. A meta-analysis of five studies comprising nearly 1,000 children found that the presence of retinal hemorrhages was associated with an odds ratio of 14.7 (95% CI: 6.39–33.62) for AHT, corresponding to a 91% probability of abuse.11 In the aggregated cohort, 84% of children with AHT had retinal findings, compared to only 9% of those with non-abusive head trauma (nAHT). Certain types of hemorrhages further strengthen this association: preretinal hemorrhages were observed in 56% of AHT cases versus 18% in nAHT, and subretinal hemorrhages were present in 40% of AHT cases but were not documented in any nAHT cases. These findings underscore the high diagnostic value of retinal findings in the context of suspected AHT.
Workup and Multidisciplinary Evaluation
Cases of abusive head trauma often require multidisciplinary care involving teams such as neurology, neurosurgery, emergency medicine, trauma, ophthalmology, orthopedics, and the pediatric intensive care unit. In addition, comprehensive evaluation includes collaboration with social work, child protection services, and the hospital’s Safe Family team to assess for child abuse and neglect.
Management and Outcome
Sequelae of abusive head trauma can be severe and long-lasting. Ocular complications may range from complete resolution of retinal hemorrhages to central vision loss and optic atrophy, which can result from elevated intracranial pressure or direct intraocular axonal injury. Additional, subretinal neovascular membrane formation has been reported, potentially leading to progressive vision loss if not identified and managed appropriately. Given these risks, long term ophthalmologic follow-up is an essential component of care, as early identification and management of visual impairments can significantly impact developmental outcomes and quality of life.
Case Presentation
A 6-week-old infant, born at 34-week gestation, presented to the emergency department with seizure like activity. Mother reported that the patient was in his usual state of health until this morning. Last night, the child’s father cared for him and noted he was unusually difficult to soothe and did not wake up for his usual feeds. When he did wake, he fed poorly and cried persistently. Over the day, the mother noted worsening symptoms including poor feeding, increased sleepiness, and reduced interaction. Home monitoring device showed that the patient’s heart rate was 90-100 bpm, lower than usual. The infant was taken to his PCP, where arm twitching and foot twitching were noticed. The mother was advised to bring the infant to ER for concerns for seizures. Per parents, no fevers, vomiting, cough, congestion, rhinorrhea, or sick contacts were reported.
At the ED, the patient received infectious workup and a head ultrasound, which revealed bilateral subdural hematomas concerning for abusive head trauma. There was bruising noted on the patient’s side and buttocks. The patient was intubated due to seizure activity and GCS of 5.
Head imaging including CT head w/o contrast and Brain MRI found diffuse restricted diffusion, consistent with hypoxic ischemic injury, no apparent intraparenchymal hemorrhages, diffuse bilateral supratentorial and infratentorial subdural hemorrhages with minimal intraventricular hemorrhage, and subgaleal fluid collection.
Ophthalmology was consulted for suspected nonaccidental trauma, and dilated fundus exam revealed extensive preretinal, intraretinal and subretinal hemorrhages extending to the ora serrata in each eye. Laboratory work-up did not reveal evidence of a bleeding disorder or other pathology that could explain extensive retinal hemorrhages. Skeletal survey was normal.
Differential Diagnosis
Non-accidental trauma, accidental trauma, seizures, bleeding disorders (hemophilia, Vitamin K deficiency, thrombocytopenia), sepsis/disseminated intravascular coagulation, metabolic disorders, infectious and inflammatory disorders (meningitis/encephalitis)
Prognosis and long-term management
Outpatient follow up with social work, neurology and ophthalmology.
References:
- Narang SK, Haney S, Duhaime AC, et al. Abusive Head Trauma in Infants and Children: Technical Report. Pediatrics. 2025;155(3):e2024070457. doi:10.1542/peds.2024-070457
- Joyce T, Gossman W, Huecker MR. Pediatric Abusive Head Trauma. In: StatPearls. StatPearls Publishing; 2025. Accessed June 28, 2025. http://www.ncbi.nlm.nih.gov/books/NBK499836/
- Parks SE, Annest JL, Hill HA, Karch DL. Pediatric abusive head trauma : recommended definitions for public health surveillance and research. Accessed June 28, 2025. https://stacks.cdc.gov/view/cdc/26243
- Rebbe R, Mienko JA, Martinson ML. Incidence and Risk Factors for Abusive Head Trauma: A Population-Based Study. Child Abuse Rev. 2020;29(3):195-207. doi:10.1002/car.2630
- Nuño M, Shelley CD, Ugiliweneza B, Schmidt AJ, Magaña JN. Differences in Incidence and Case Fatality of Abusive Head Trauma. Child Abuse Negl. 2020;104:104488. doi:10.1016/j.chiabu.2020.104488
- Hung KL. Pediatric abusive head trauma. Biomedical Journal. 2020;43(3):240-250. doi:10.1016/j.bj.2020.03.008
- Pinto PS, Meoded A, Poretti A, Tekes A, Huisman TAGM. The unique features of traumatic brain injury in children. review of the characteristics of the pediatric skull and brain, mechanisms of trauma, patterns of injury, complications, and their imaging findings–part 2. J Neuroimaging. 2012;22(2):e18-41. doi:10.1111/j.1552-6569.2011.00690.x
- Harris CK, Stagner AM. The Eyes Have It: How Critical are Ophthalmic Findings to the Diagnosis of Pediatric Abusive Head Trauma? Semin Ophthalmol. 2023;38(1):3-8. doi:10.1080/08820538.2022.2152712
- Shaken Baby Syndrome: Making an Accurate Diagnosis. American Academy of Ophthalmology. May 1, 2014. Accessed June 28, 2025. https://www.aao.org/eyenet/article/shaken-baby-syndrome-making-accurate-diagnosis
- Lantz PE, Sinal SH, Stanton CA, Weaver RG. Perimacular retinal folds from childhood head trauma. BMJ. 2004;328(7442):754-756. doi:10.1136/bmj.328.7442.754
- Maguire SA, Watts PO, Shaw AD, et al. Retinal haemorrhages and related findings in abusive and non-abusive head trauma: a systematic review. Eye (Lond). 2013;27(1):28-36. doi:10.1038/eye.2012.213
Copyright statement: Copyright Alvina Liang, Theresa Long, ©2025. For further information regarding the rights to this collection, please visit: URL to copyright information page on Moran CORE
Other images: