


EYELIDS
Home / Ophthalmic Pathology / Eyelids
Macroscopic Overview –Normal Eyelid:
The eyelid is comprised of several layers of tissue derived from surface ectoderm. From anterior to posterior, the layers are as follows: Skin, Muscle, Tarsus, and Conjunctiva.
- Skin: keratinized stratified squamous epithelium with melanocytes, thinnest skin in the body
- Does not have a true dermis, therefore there are no rete ridges or pegs
- Dermal appendages: small fine hairs, eccrine glands, apocrine glands (of Moll), sebaceous glands (of Zeiss)
- Muscle: Orbicularis oculiis a “C” shape with the nasal side open
- Has three components: pretarsal (anterior to tarsus), preseptal (superior to tarsus and anterior to septum), and orbital
- Tarsus: dense fibrous connective tissue layer that houses meibomian glands and the accessory lacrimal glands of Wolfring
- In rats and rabbits, the tarsus contains cartilage; however, no cartilage in the tarsus of primates
- Conjunctiva: Palpebral conjunctiva
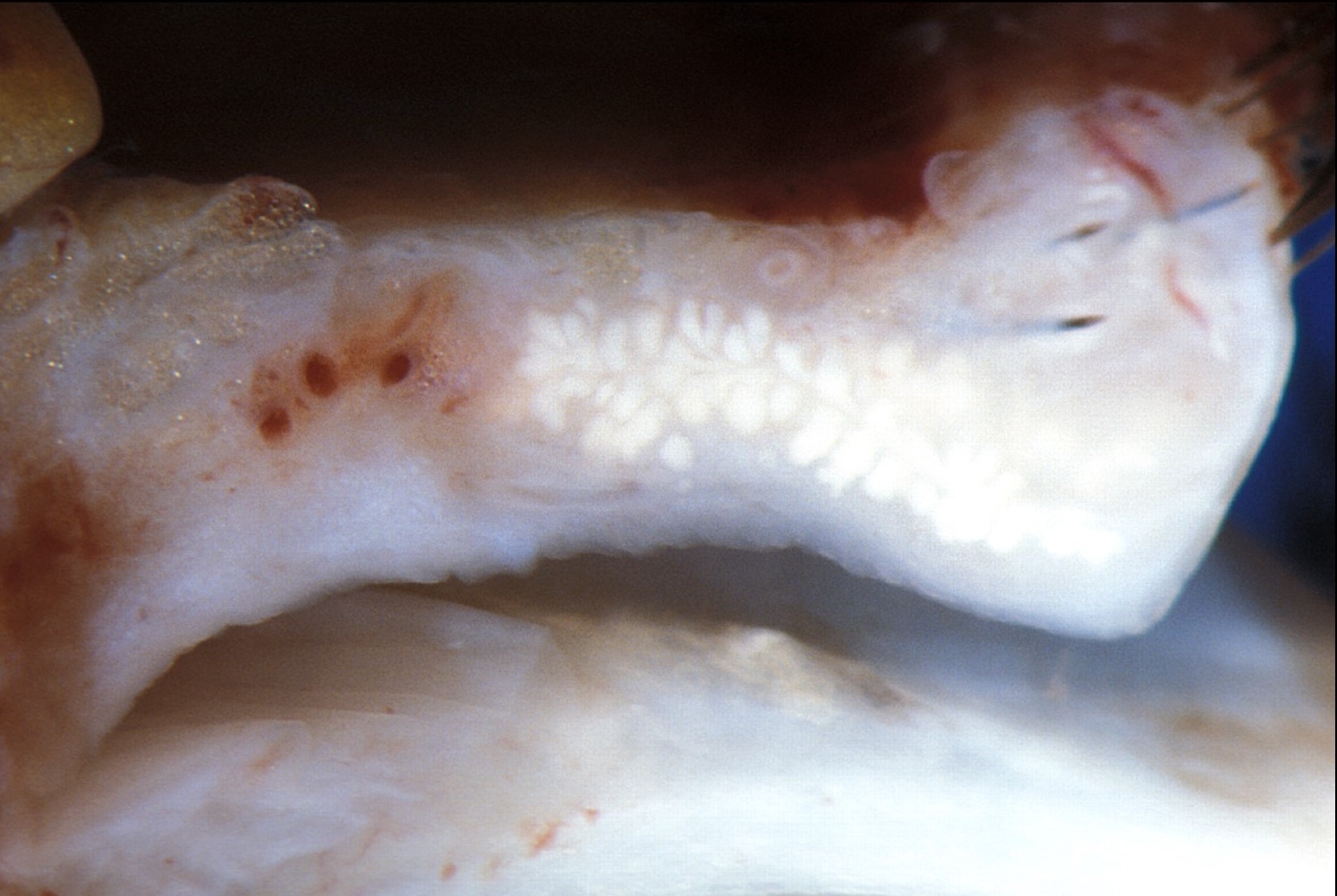

Gross cross-section of eyelid


Trichrome stain of eyelid cross-section
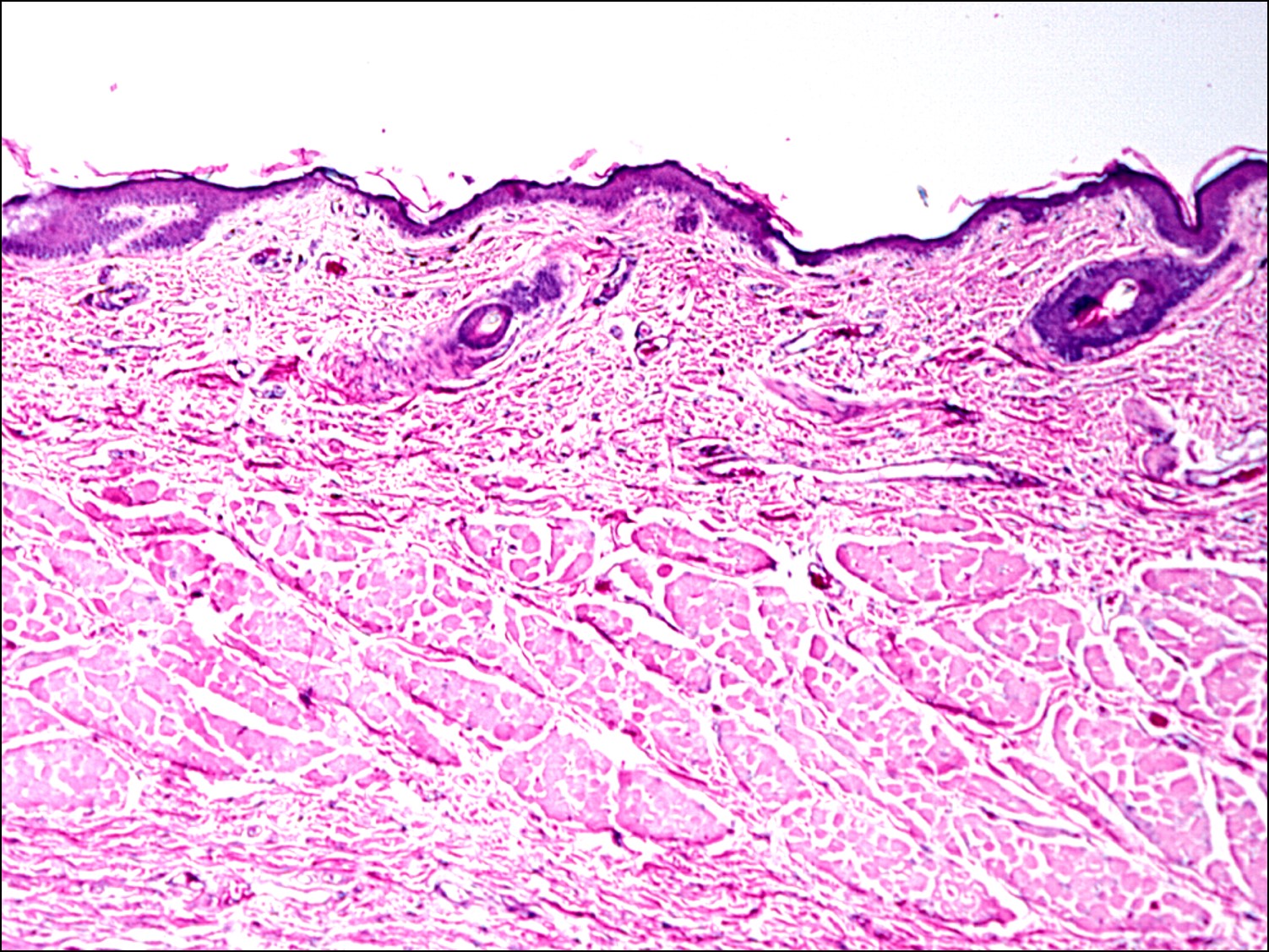
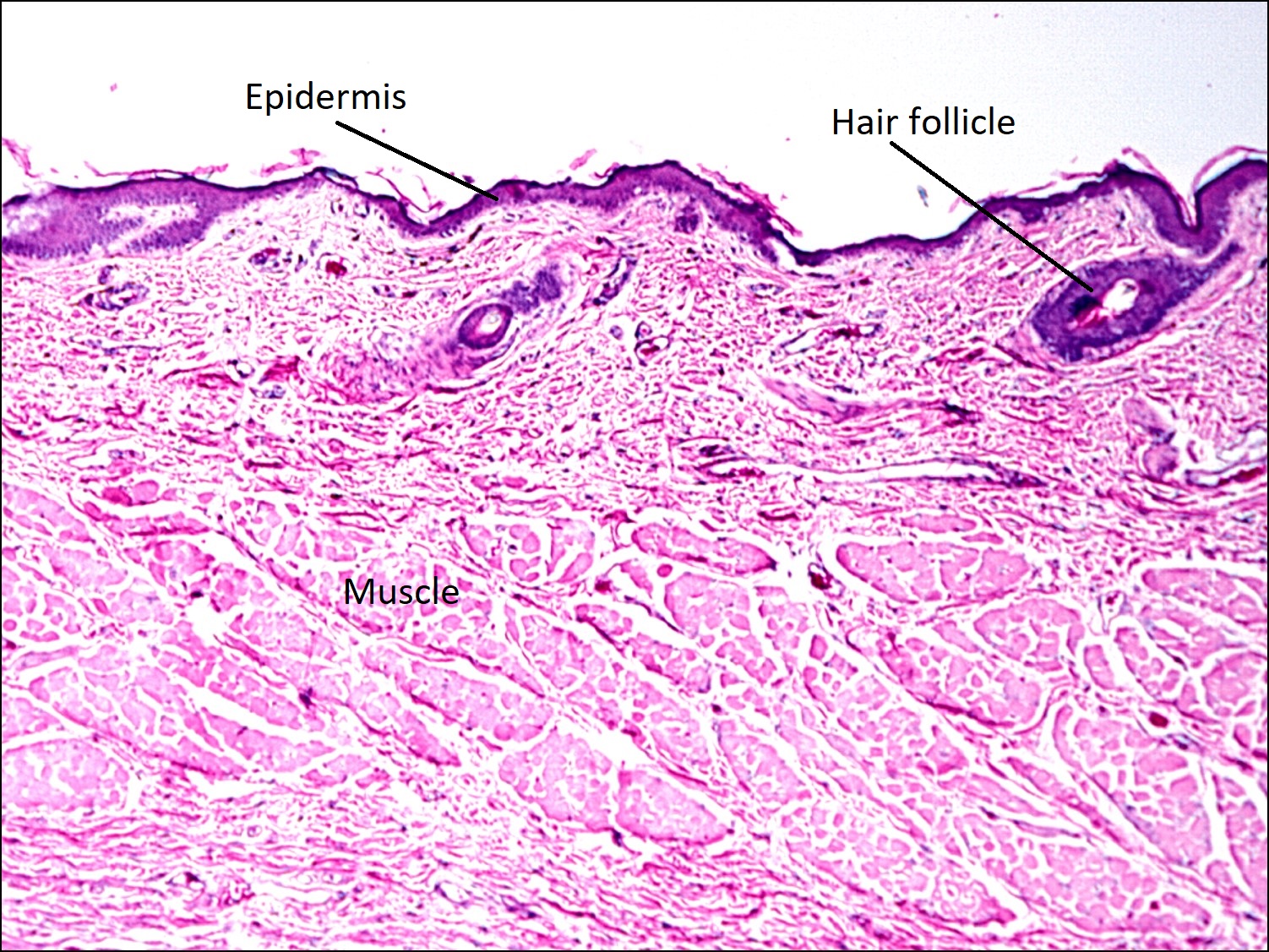
H&E stain of eyelid
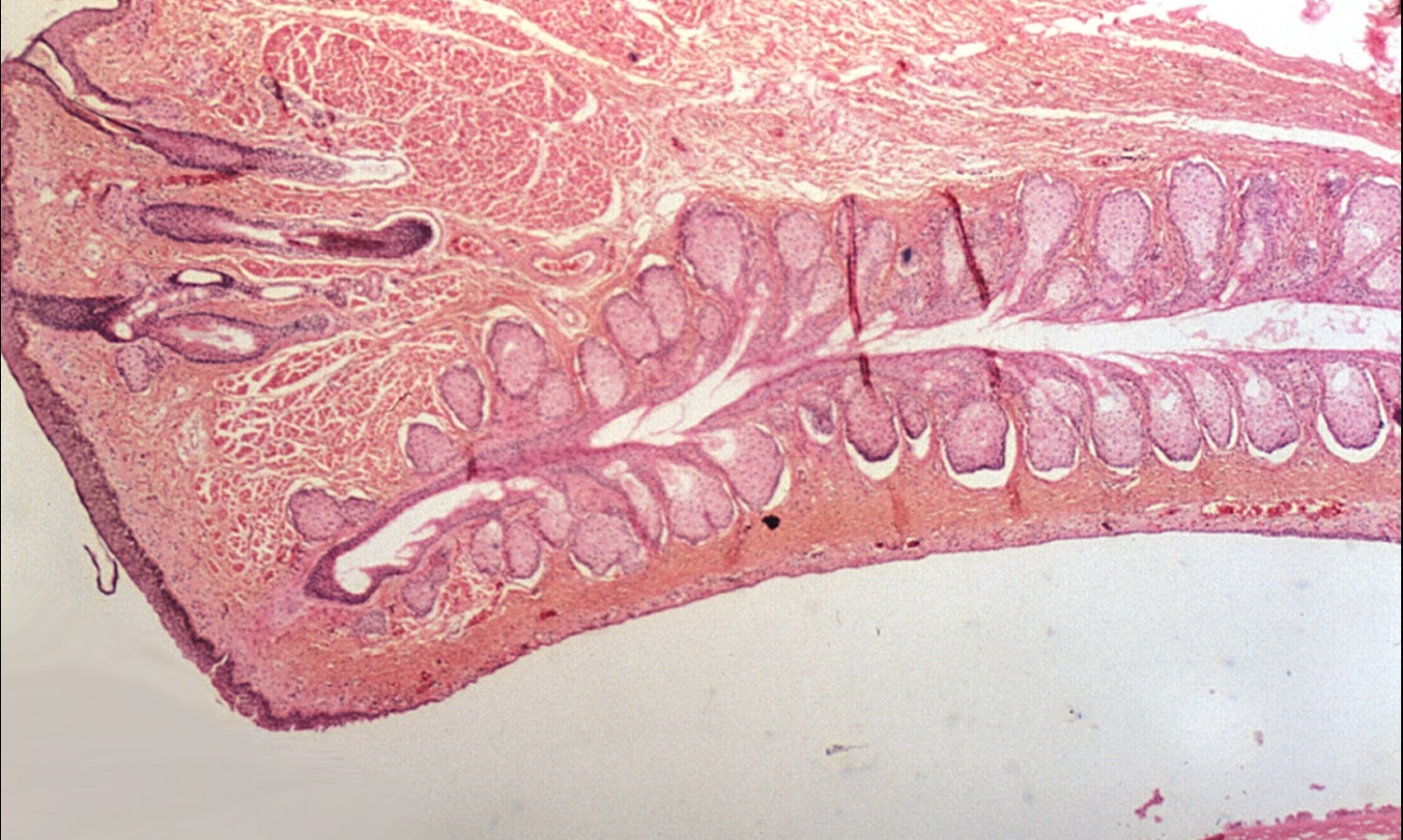
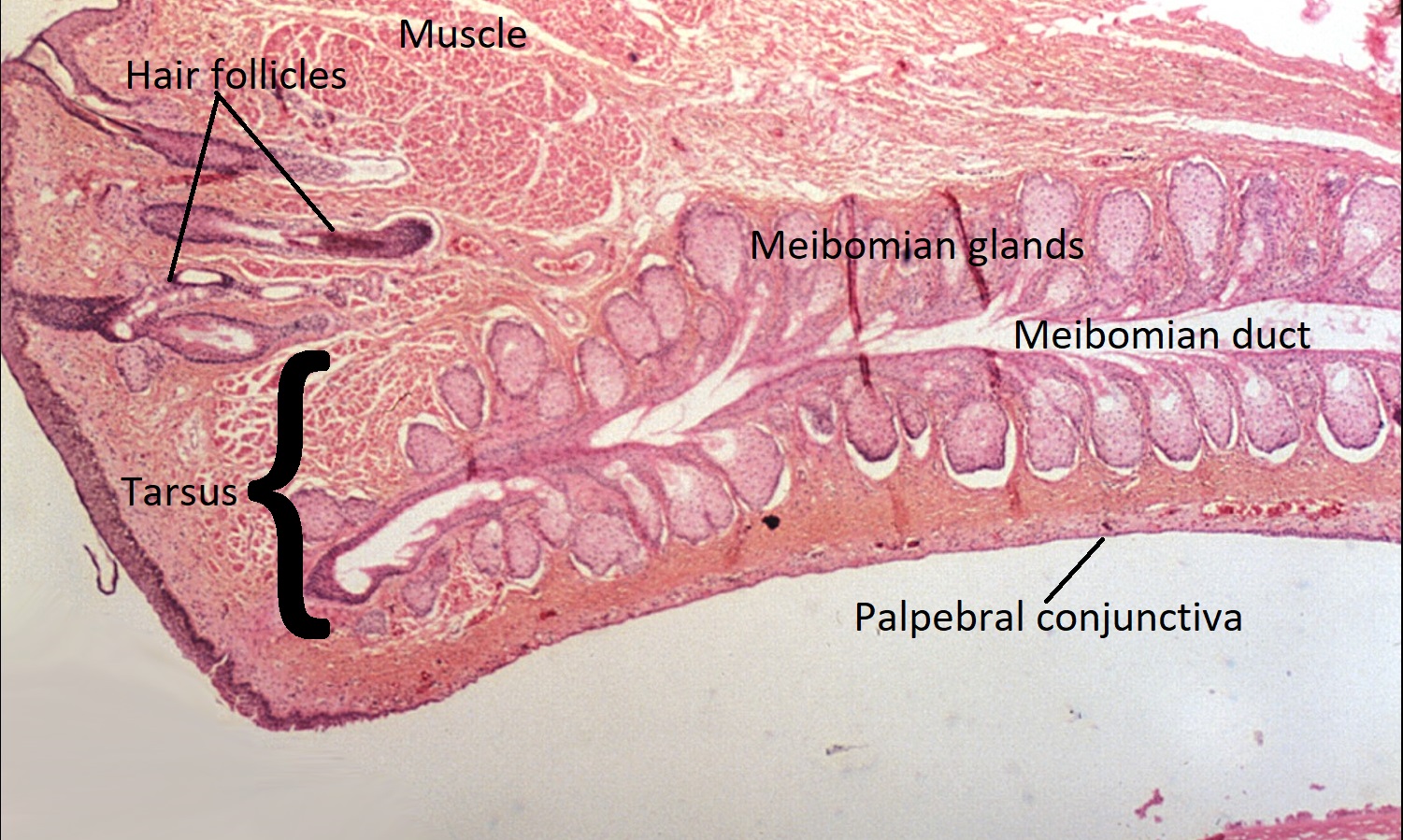
Tarsus and meibomian glands
Several dermatopathology terms are applicable to eyelid pathology.
- Acanthosis: thickened squamous epithelium, particularly in stratum spinosum
- Dyskeratosis: keratinization of normally nonkeratinized cells, particularly within stratum spinosum
- Hyperkeratosis: excess superficial keratin layer(stratum corneum and granulosum)
- Parakeratosis: retained nuclei present in superficial keratin layer(stratum corneum) and absent stratum granulosum


Acanthosis

Dyskeratosis


Hyperkeratosis
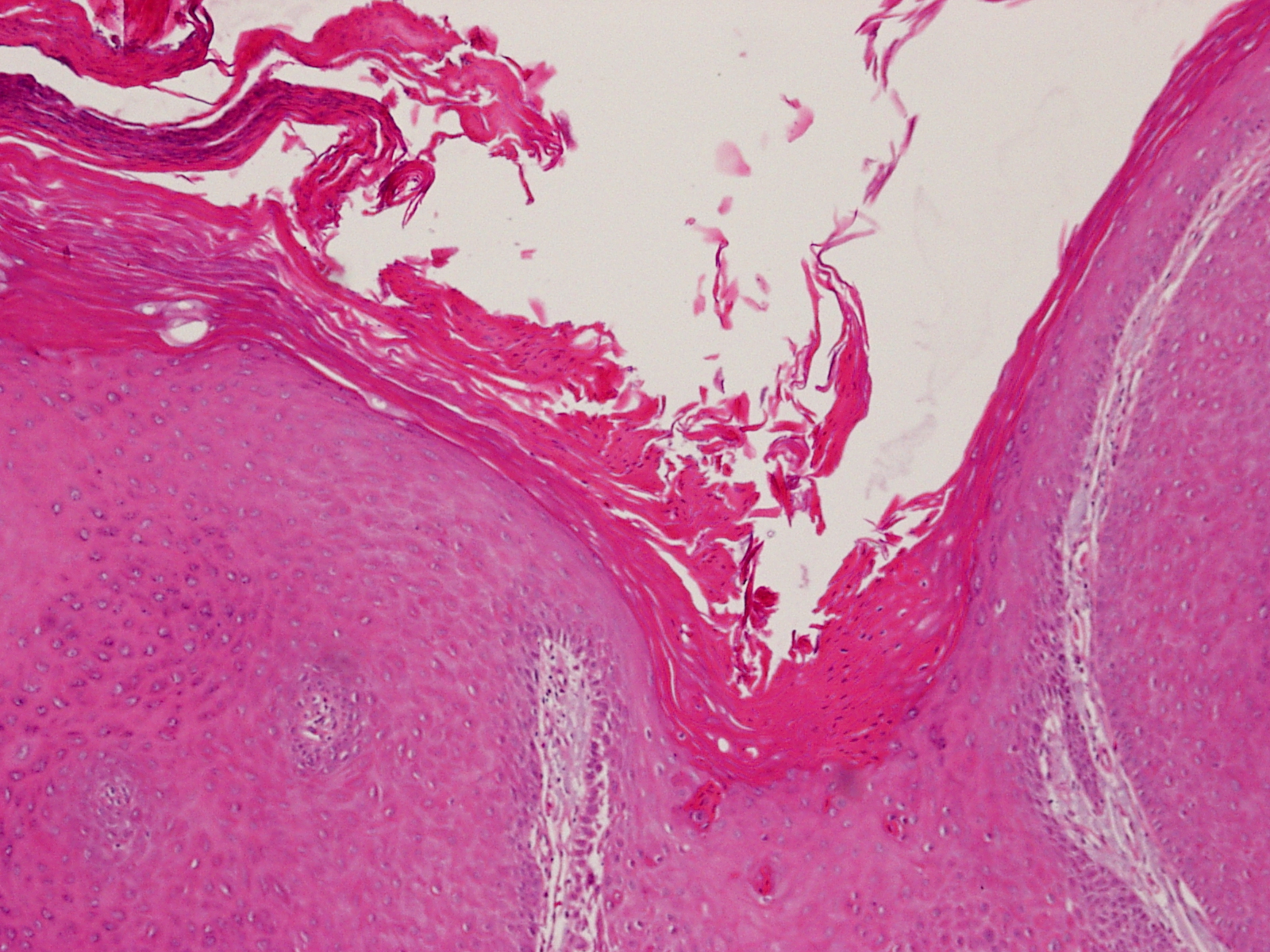
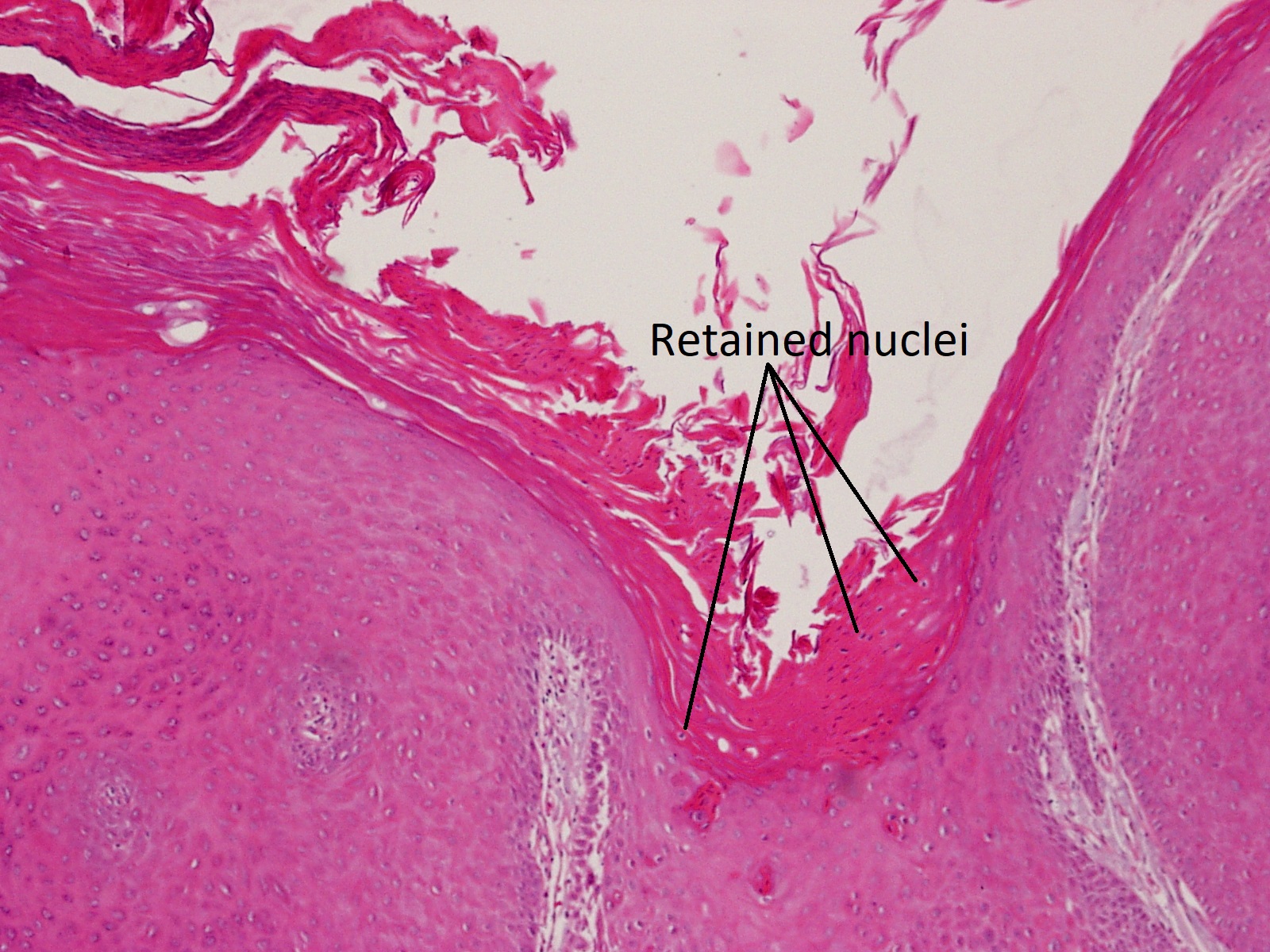
Parakeratosis
All three general types of glands are present in the eyelid. The lid margin contains a higher concentration of these glands.
- Eccrine: secrete via exocytosis (secretory vessels coalesce with apical membrane and release product)
- Clusters of acini empty into a central lumen
- Secretory cells have eosinophilic granules in their cytoplasm
- Examples: sweat glands, lacrimal gland
- Accessory Lacrimal Gland of Krauss: empties into the fornix
- Accessory Lacrimal Gland of Wolfring: in the tarsus
- Apocrine: secrete by pinching off apical portion of cell into lumen, cells have projections on microscopy
- Produce oily secretions
- Glands of Moll: secrete onto hair cell at lid margin
- Tip: Mispronounce as Mole because moles have snouts and apocrine cells have projections.
- Holocrine: secrete products when entire cell breaks apart (“kamikaze” secretion)
- Central nucleus with foamy cytoplasm
- Meibomian Glands: in the tarsus, empties at gray line of lid margin
- Secretes oily layer of tear film
- Glands of Zeiss: secrete onto eyelash hair shaft
- Same as sebaceous glands attached to normal hair. Only called glands of Zeiss when attached to eyelashes.
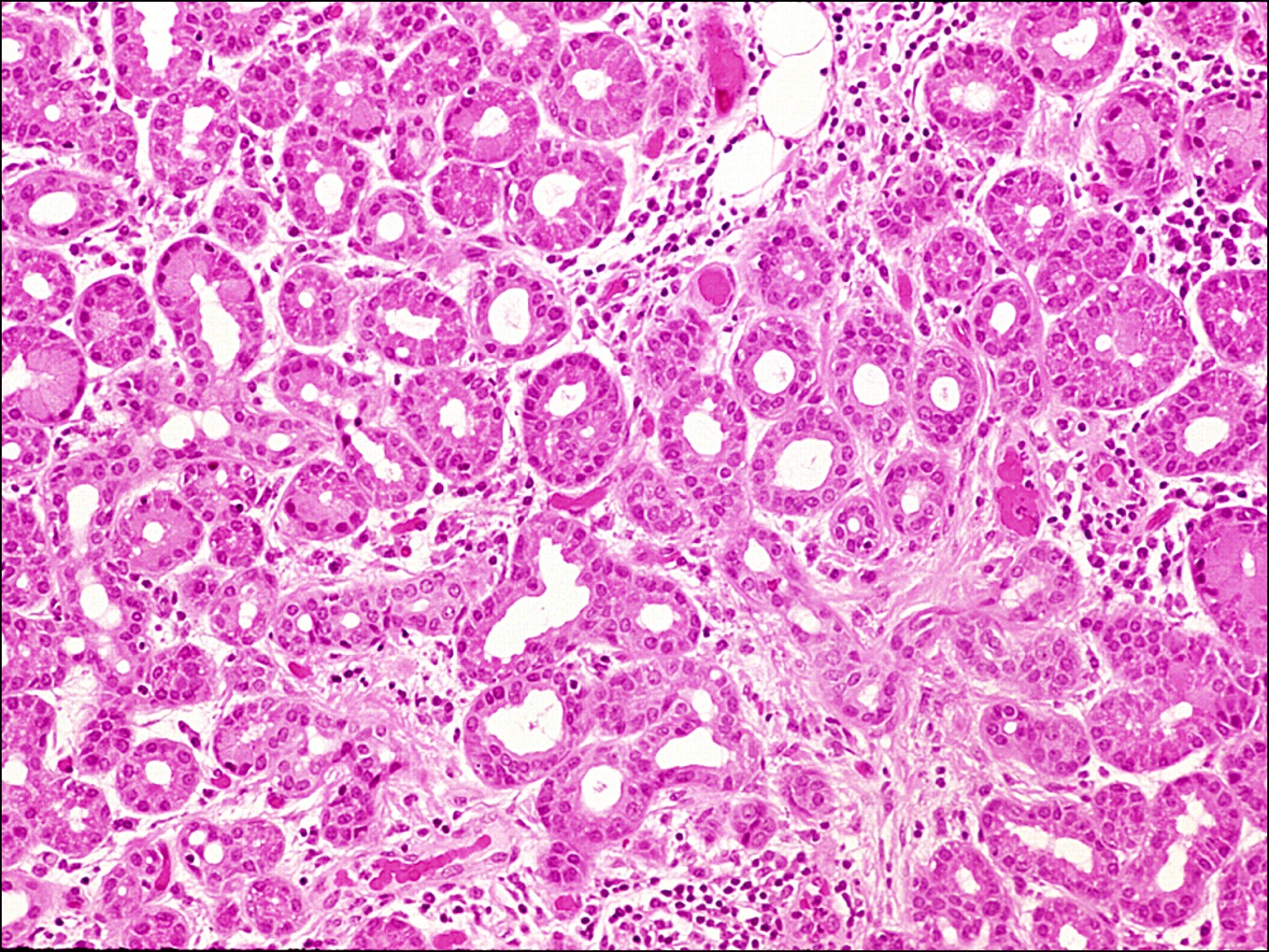

Eccrine-type lacrimal glands
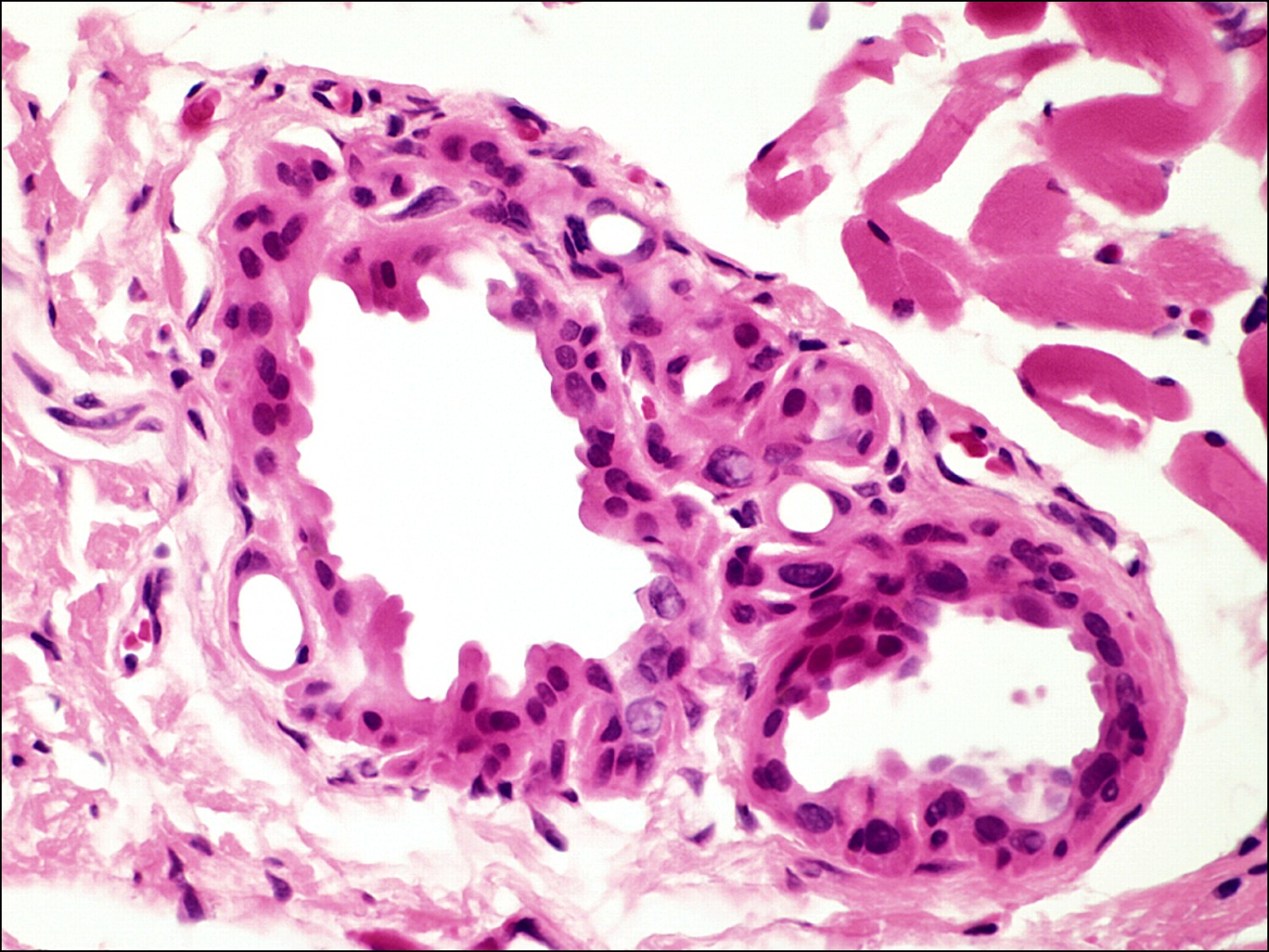

Apocrine glands of Moll

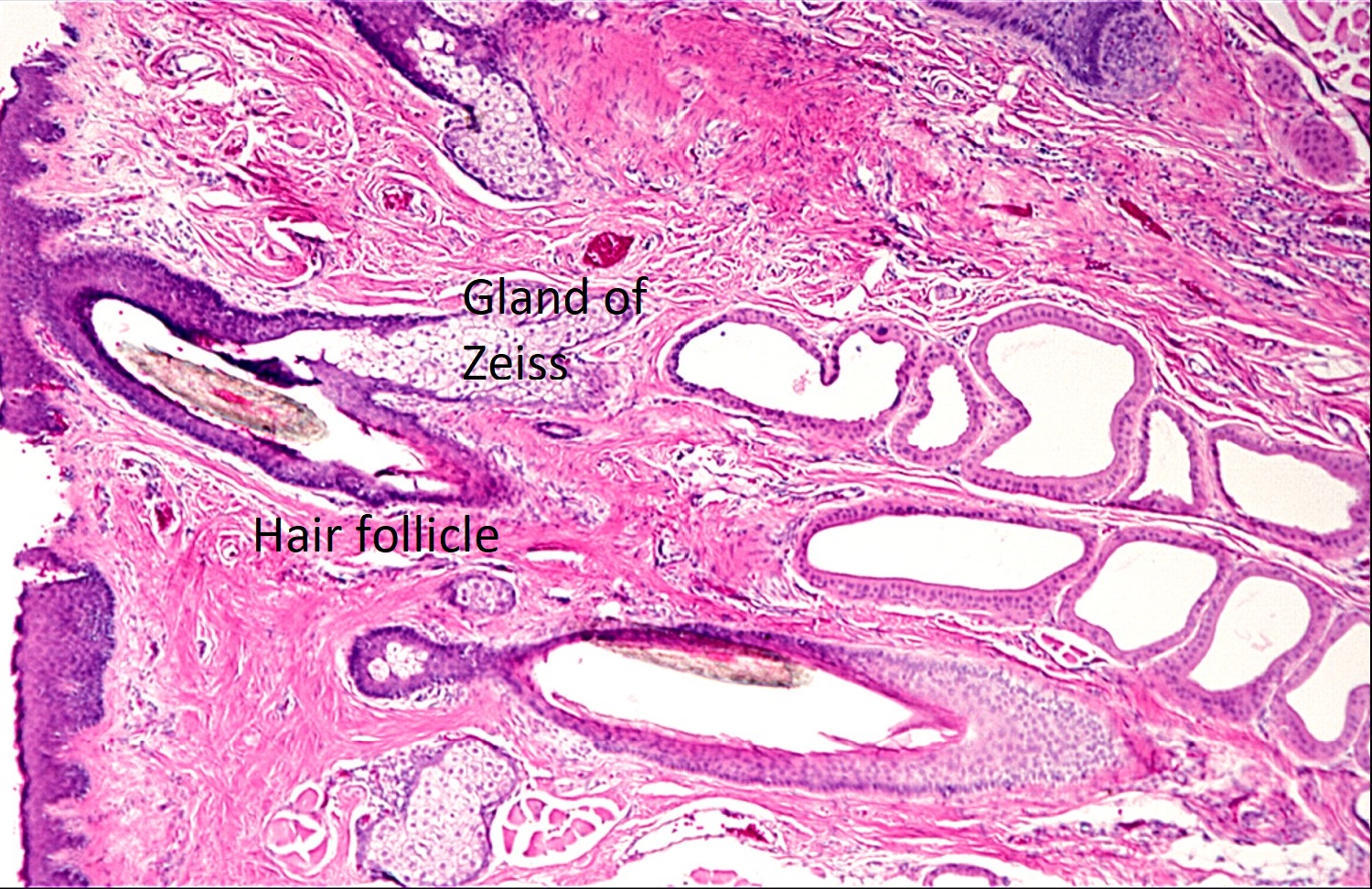
Eyelashfollicle with sebaceous glands of Zeiss
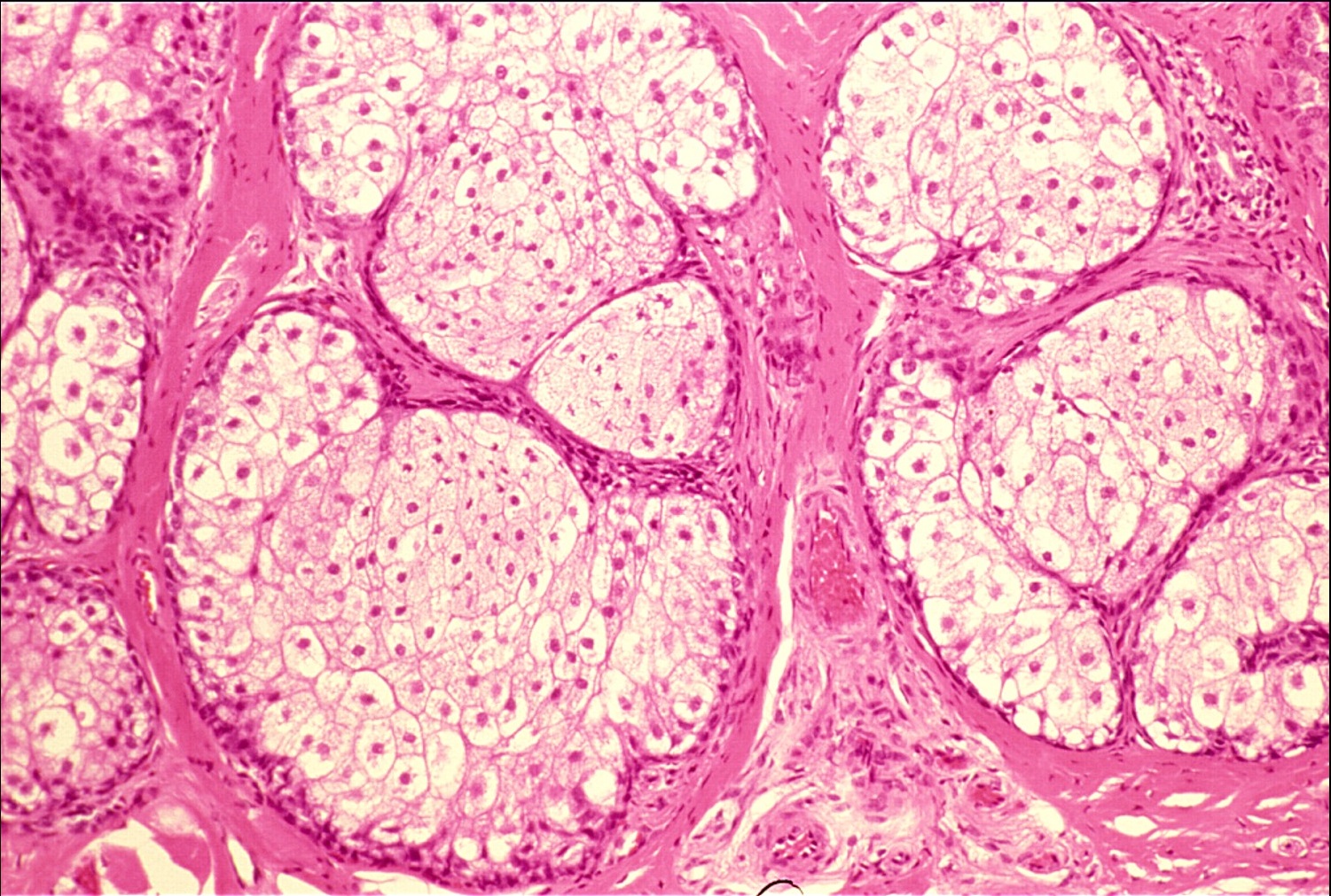

Sebaceous Meibomian glands
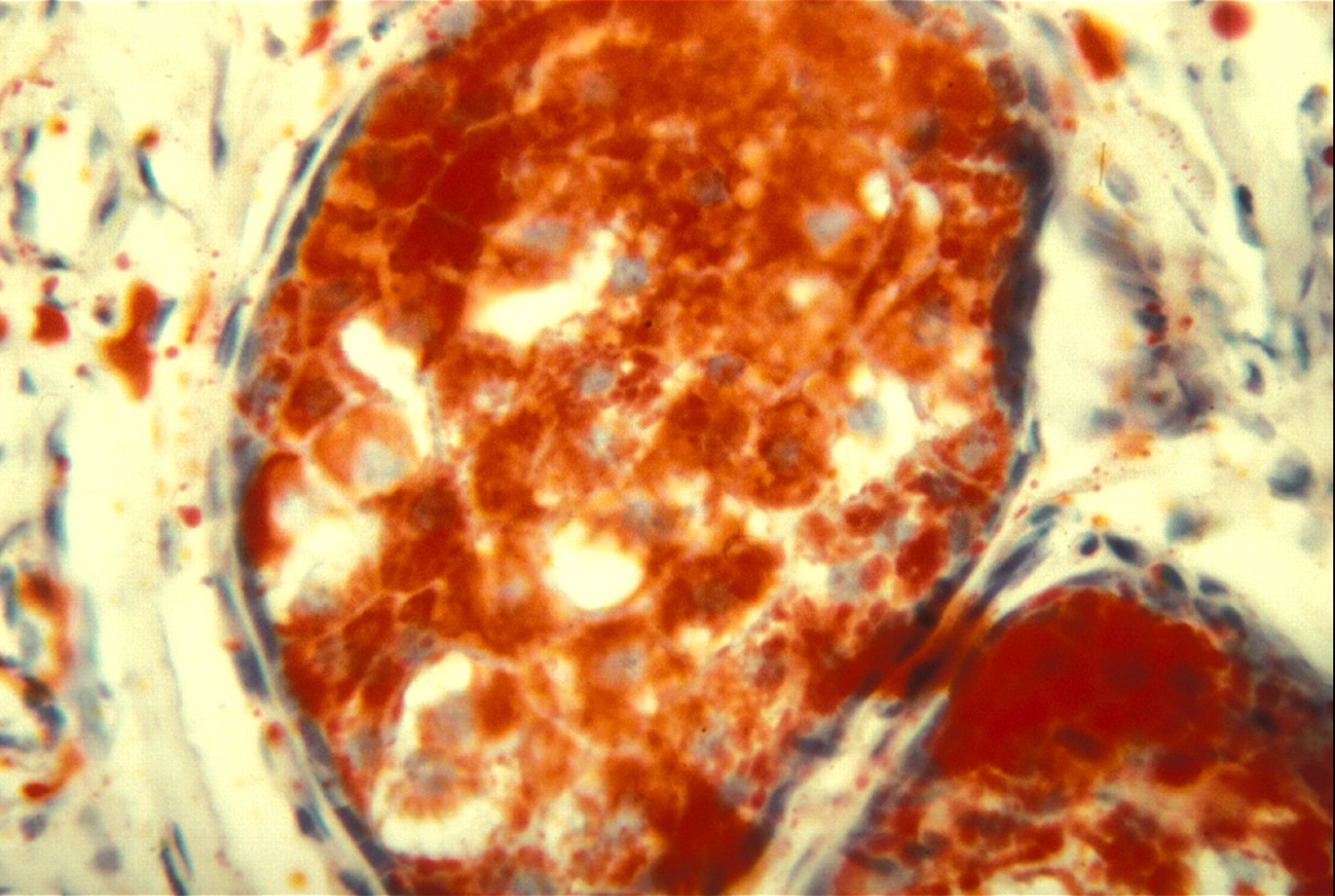

Oil Red O Stain


Lid margin with several glands
Distichiasis
- Congenital, usually autosomal dominant, condition in which the eyelashes exit through the ducts of meibomian glands.
- Two rows of eyelashes
- Thought to be an erroneous formation of a complete pilosebaceous unit instead of a normal meibomian gland.
- Often associated with Trisomy 18 and mandibulofacial dystosis
Bacterial Infection
- May be due to a bite or wound, contiguous spread from a sinus infection, or hematogenous dissemination
- Common pathogens
- Bacterial: Staphylococcusaureus in hordeolum and infectious blepharitis
- Viral: molluscum contagiosum
- Fungal: blastomycosis, coccidiomycosis, aspergillosis
Hordeolum

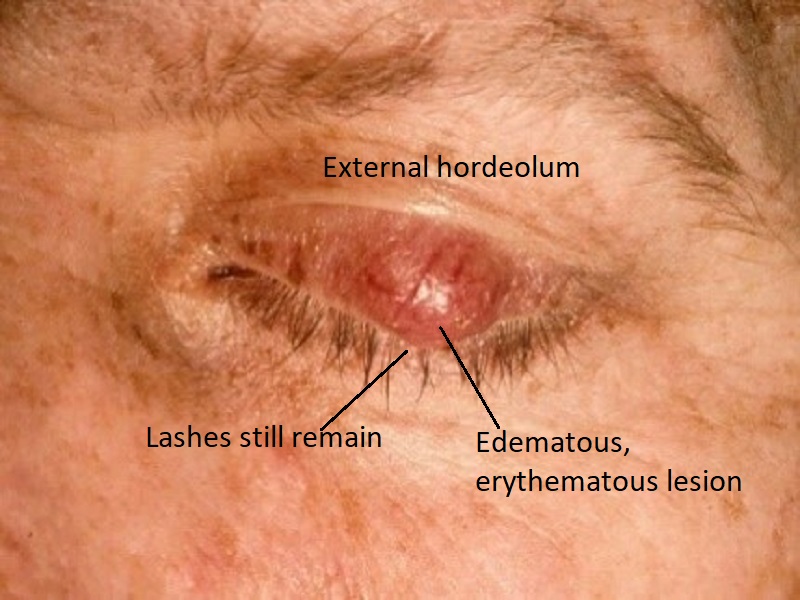
External photo
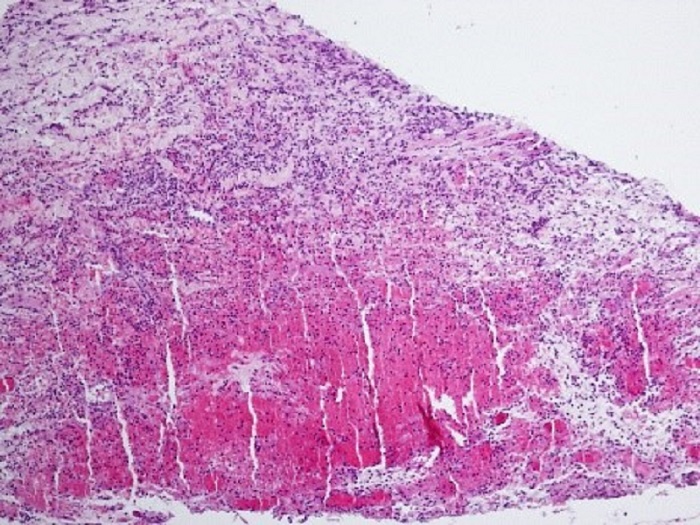

Hordeolum
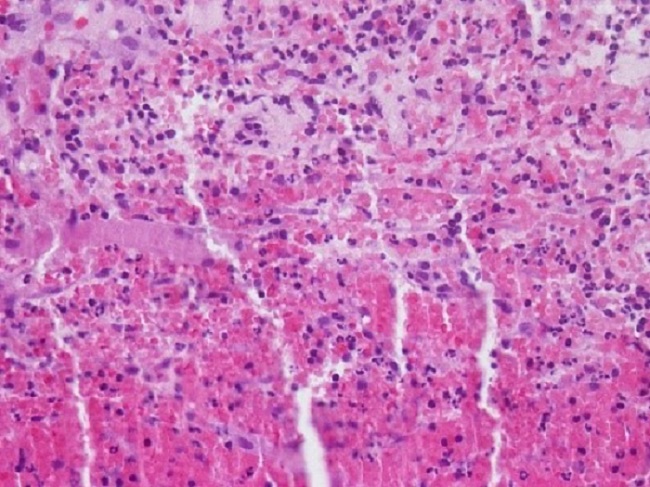

Acute Inflammatory Infiltrate
- Infection of glands of Zeiss or Moll (external), or less commonly, meibomian glands (internal)
- AKA Stye
- Typically due to Staphylococcusaureus infection leading to the formation of a small abscess
- An acute inflammatory infiltrate of PMNs along with edema, vascular congestion, and necrosisis seen histologically near hair follicles and glandular structures
Preseptal Cellulitis
- Anterior to the orbital septum, which connects the edge of the tarsal plates to the orbital rim
- Common in children
- Often secondary to extension of a sinusitis or skin trauma
- Inflammatory infiltrate (PMNs) seen amidst subcutaneous tissue, sometimes with edema, vascular congestion, or necrosis
- Most frequently due to bacteria, particularly Streptococcus
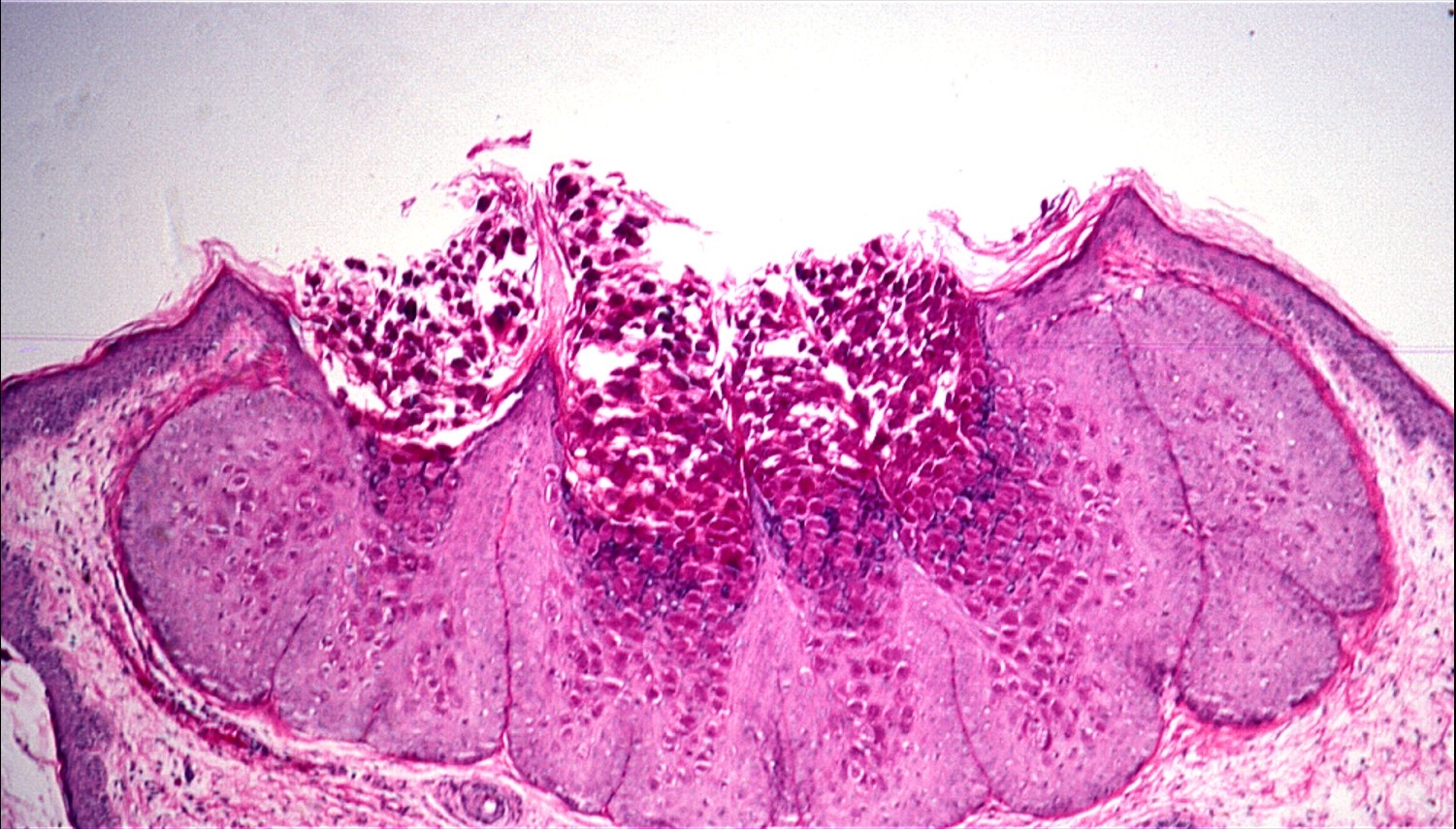
Verruca vulgaris
- Usually attributed to Human Papilloma Virus types 6 and 11
- Warty, papillomatous lesion usually near the lid margin
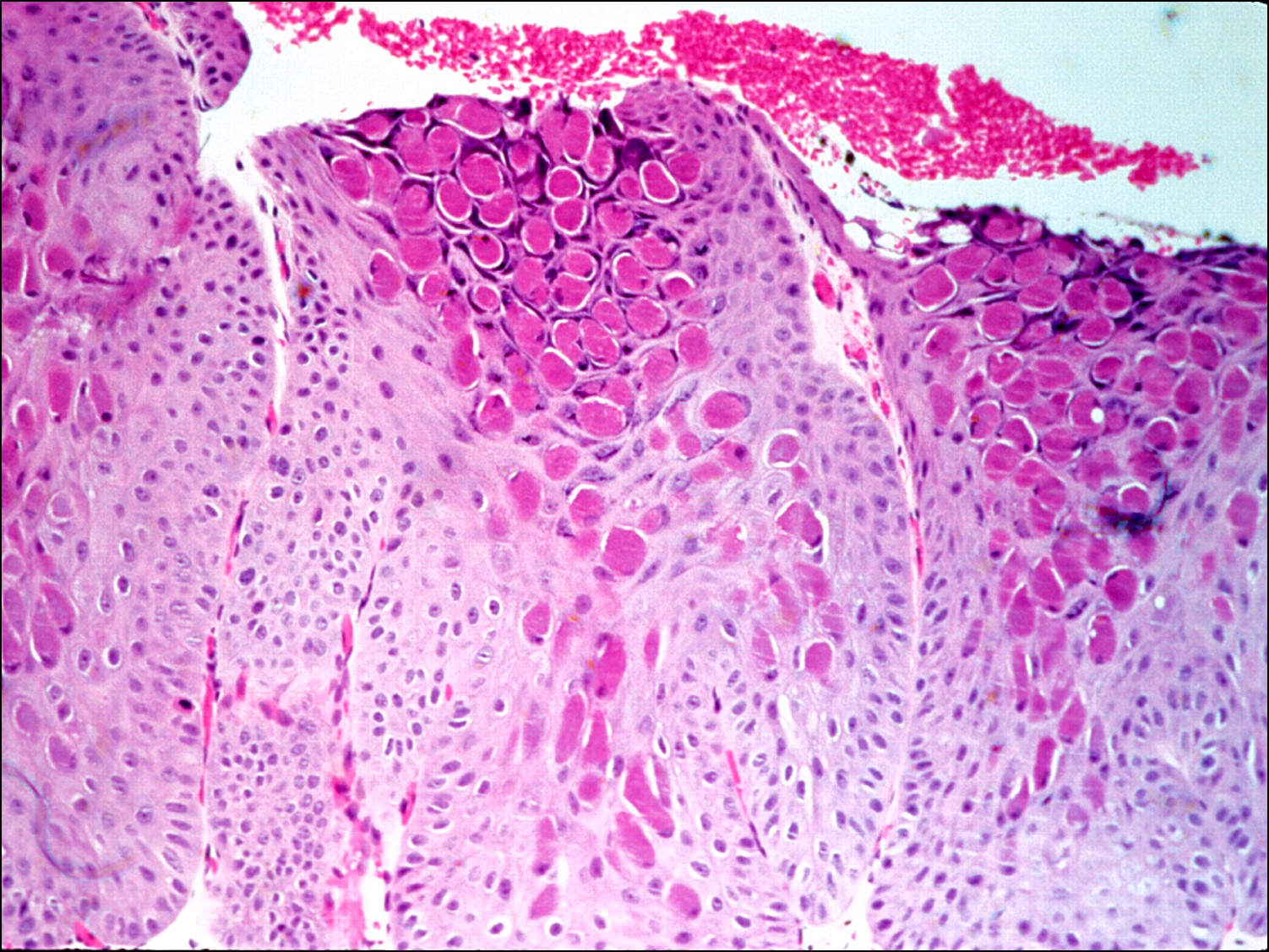
- Acanthosis, hyperkeratosis, parakeratosis, papillomatous fibrovascular cores
- Koilocytosis: larger darker-staining nucleus with a clear cytoplasm
- Infected cells occasionally show eosinophilic viral inclusion bodies
- Superficial dermis shows a mixed inflammatory infiltrate
- Can spontaneously regress
Molluscum contagiosum


External photo

Molluscum contagiosum

Viral inclusion cysts
- Caused by a pox virus
- Nodules with raised pearly border and central ulceration/umbilication
- Eosinophilic viral inclusion bodies (molluscum bodies) at basal layer move toward the center and erupt at the surface
- Acanthosis, especially at the edge of the ulcer
- Can lead to follicular conjunctivitis
Chalazion
Chalazion

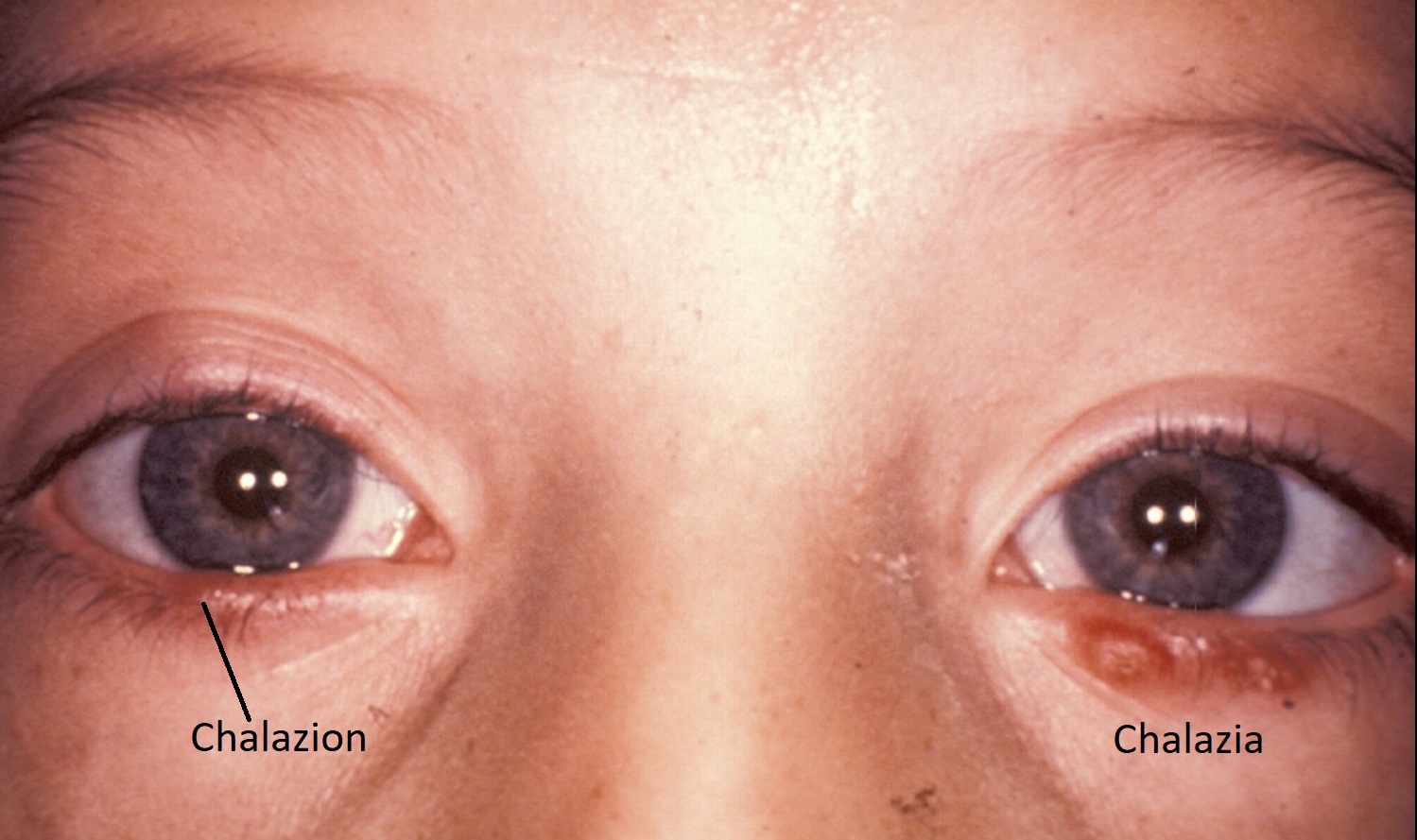
Bilateral chalazia
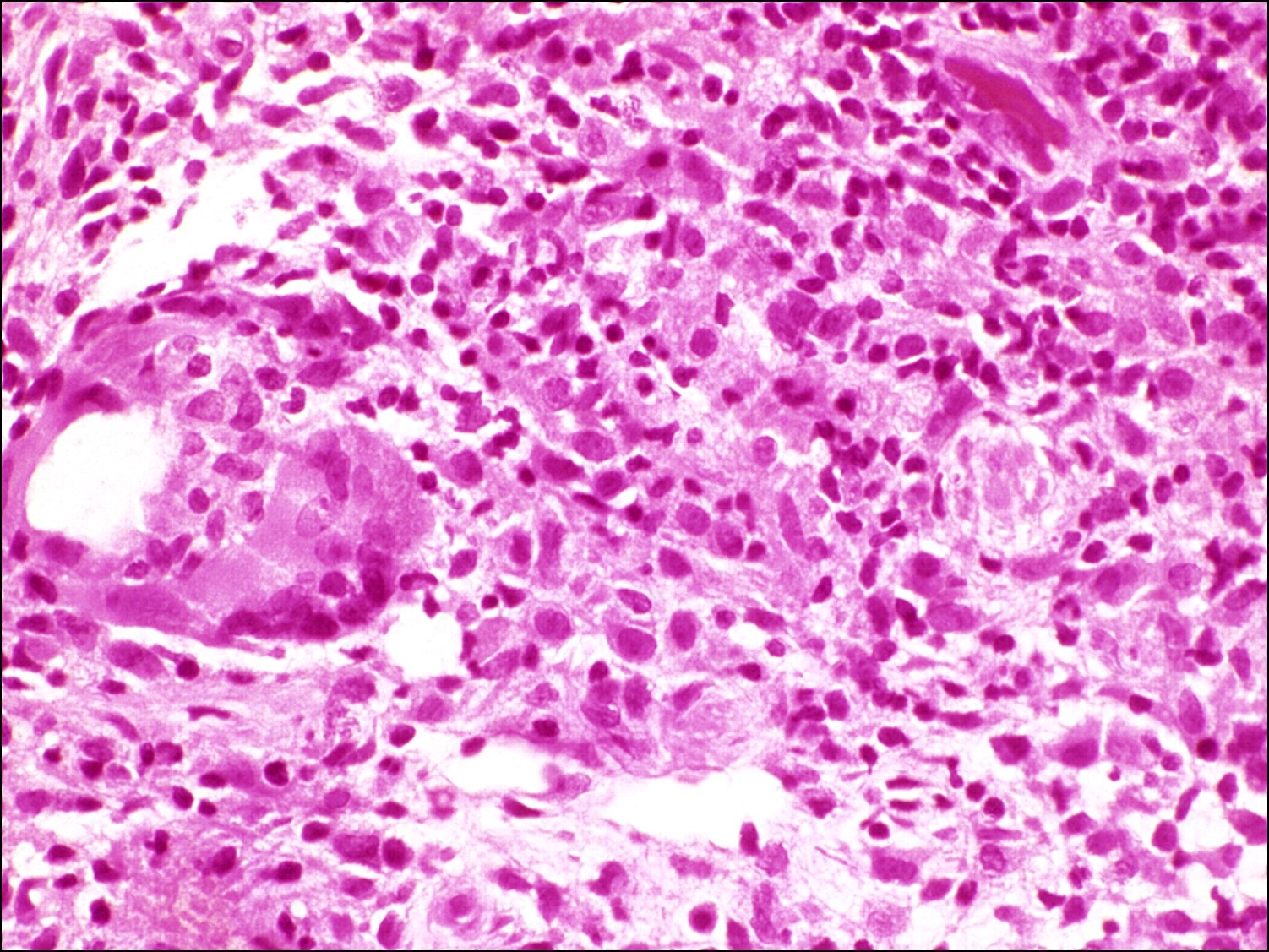

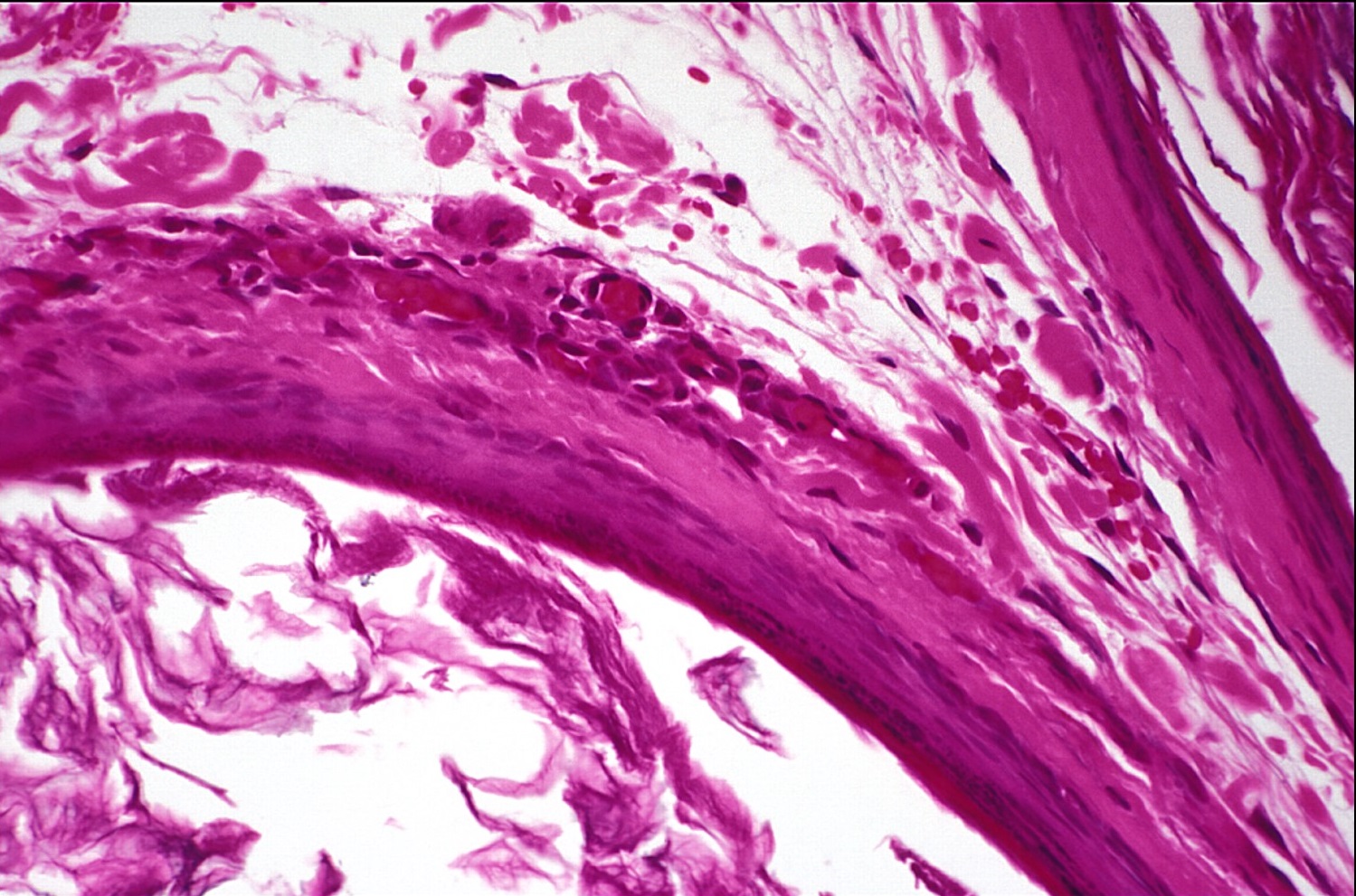
Lipogranulomatous reaction
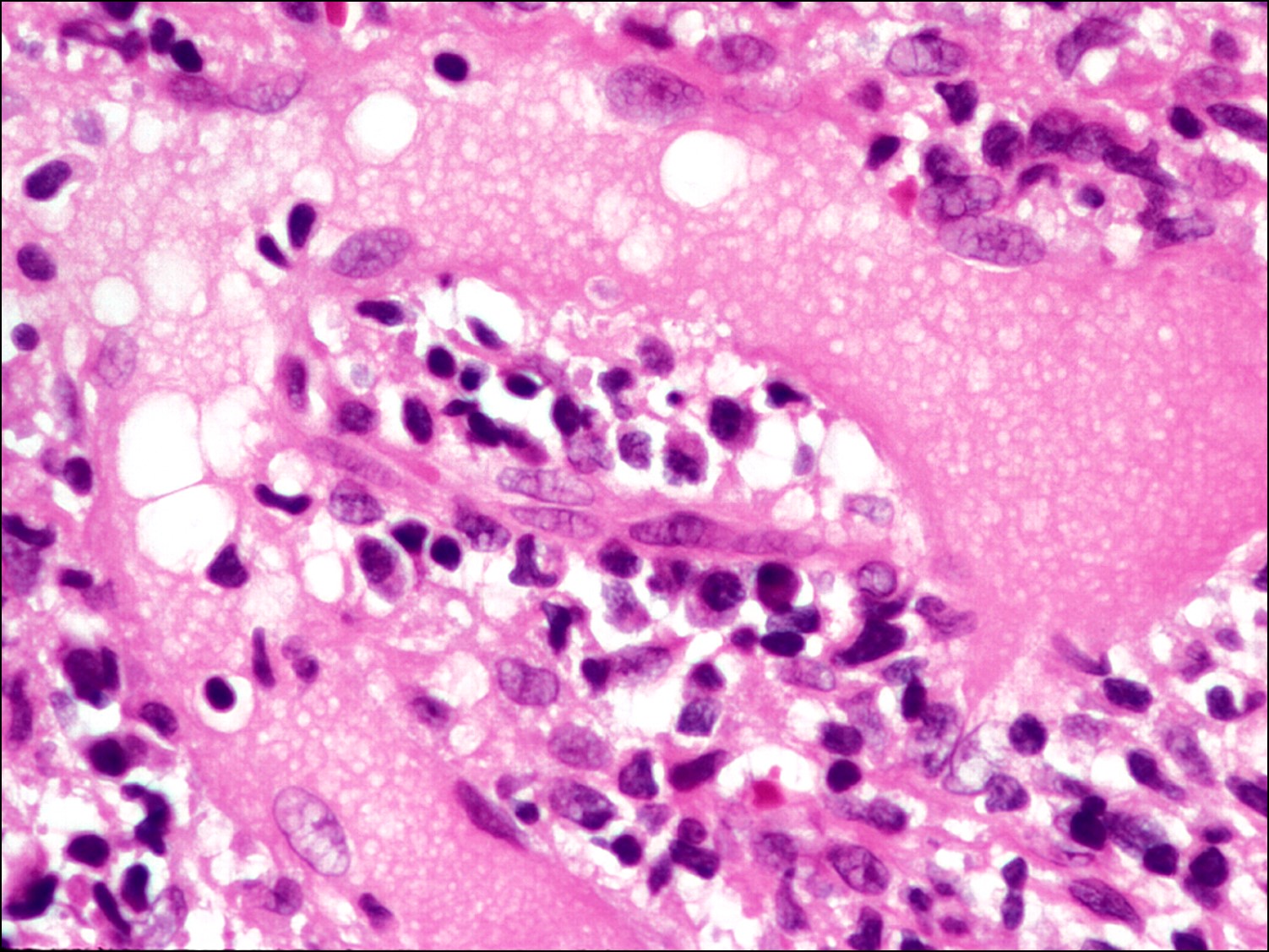

Large, lipid-laden giant cell amongst chalazion contents
- Due to backup of lipid from inspissatedmeibomian ducts
- Noninfectious lipogranulomatous mixed inflammatory reaction: giant cells, foamy macrophages, lymphocytes, plasma cells, neutrophils
- Can see lots of clear spaces from lipid droplets that do not stain with H&E
- In old lesions, additional fibrosis and scarring present
Xanthelasma


Xanthelasma
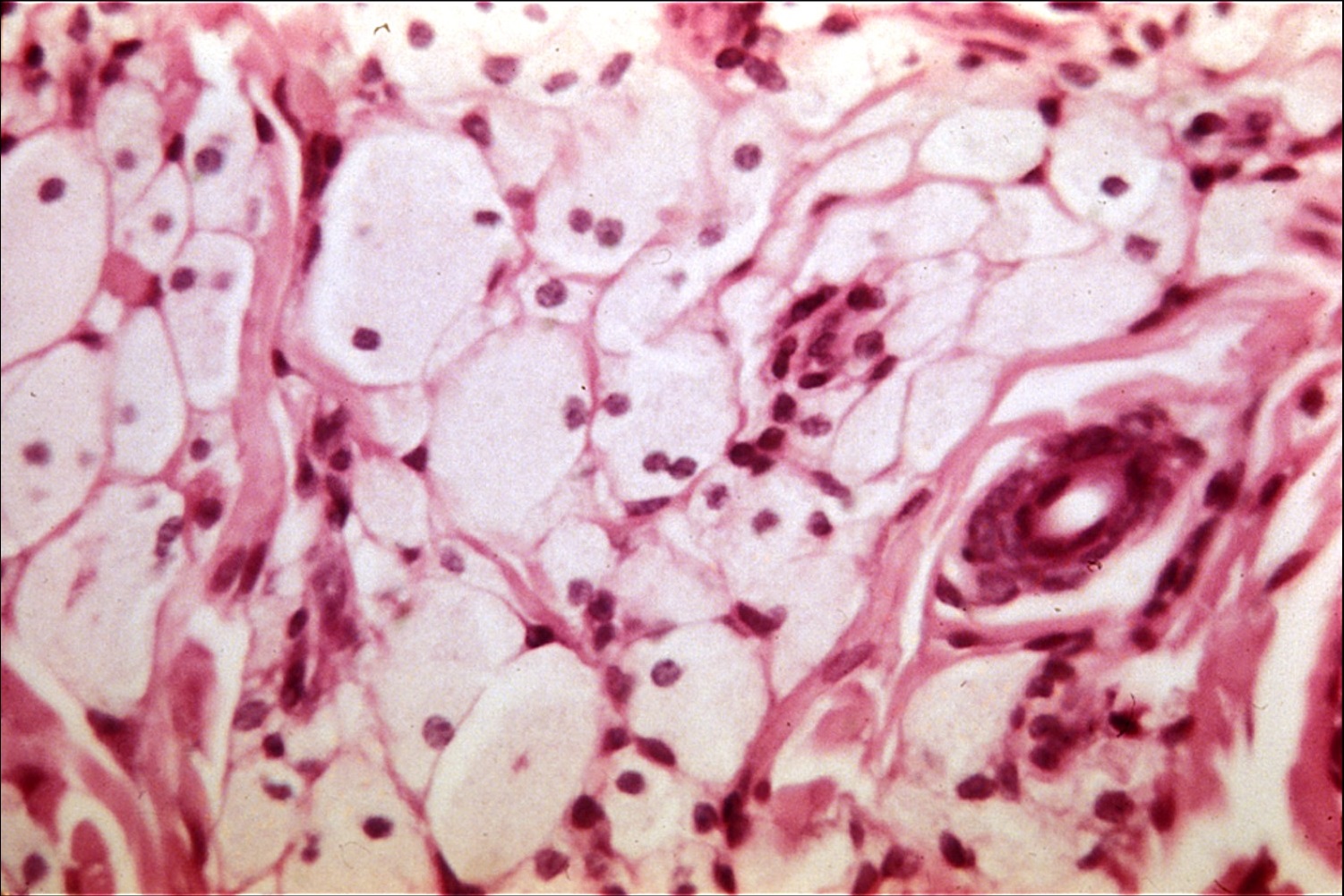

Lipid-laden histiocytes
- Yellow plaques that typically appear on the nasal side of the upper eyelids
- 30-40% of patients also have Hyperlipoproteinemia Type II or III
- Lipid-laden histiocytes with a foamy cytoplasm and central nucleus found in the superficial dermis
- As opposed to adipose cells with a peripheralnucleus
- Little to no inflammation present
Amyloid
- Numerous, bilateral, symmetric, yellowish waxy nodules
- Amorphous eosinophilic extracellular material
- Positive staining with Congo Red
- Pathognomonic apple-green birefringence under polarized light
- Amyloid deposits from
- Immunoglobulin light chain fragments: plasma cell dyscrasias
- Transthyretin mutations: Familial amyloid polyneuropathy (FAP) types I & II
- Gelsolin mutations: FAP type IV (Meretoja syndrome [Lattice Corneal Dystrophy type 2])
- Amyloid in eyelid skin strongly suggests asystemic process
Myxoma
- Rare, benign, slow-growing tumor with smooth, gelatinous appearance that is often confused with cysts
- Stellate and spindle-shaped cells with intracytoplasmic and intranuclear vacuoles
- Cells surrounded by mucoid stroma with rare reticulin and collagen fibers, resembling primitive mesenchymal tissue
Epidermoid Cyst


External photo

Keratin-filled epidermoid cyst

High magnification of cyst lining
- Cystic nodule that transilluminates on clinical exam
- Lined with stratified squamous keratinized epithelium and often contains keratin
- Often occur if a suture or previous trauma causes the epithelium to get stuck underneath
- In children, often seen with compound nevi when melanocytes pull down some epithelium with them
Dermoid Cyst


Dermoid cyst


High magnification
- Usually found in the orbit, but in the eyelid, typically located superior-temporally
- Also lined with stratified squamous keratinized epithelium
- Dermal appendages (keratin, hair follicles, sebaceous glands, eccrine glands) can be found in the wall and/or the cyst cavity itself
- Lumen can contain keratin as well as hair and sebum
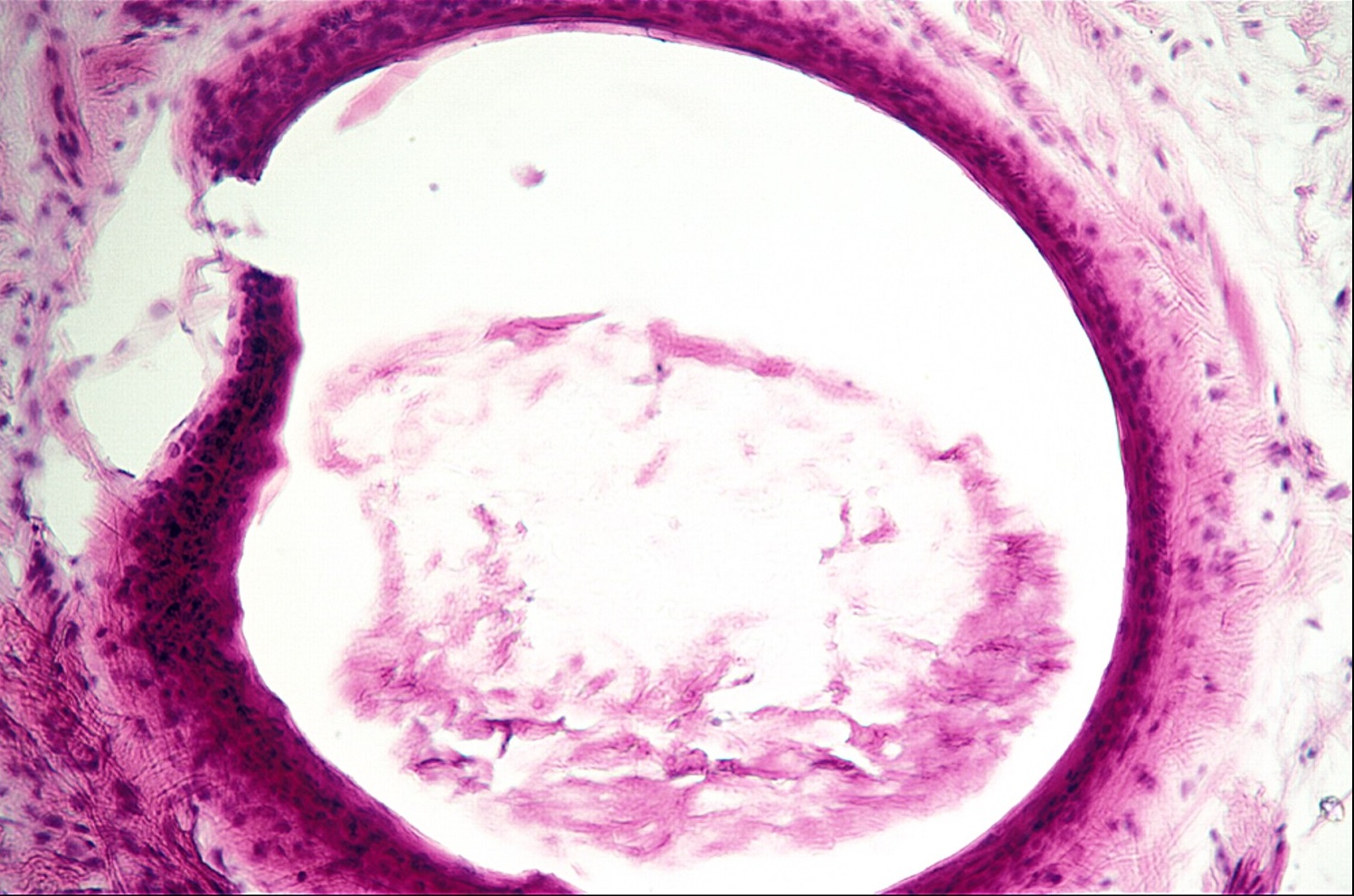
Eccrine Hydrocystoma

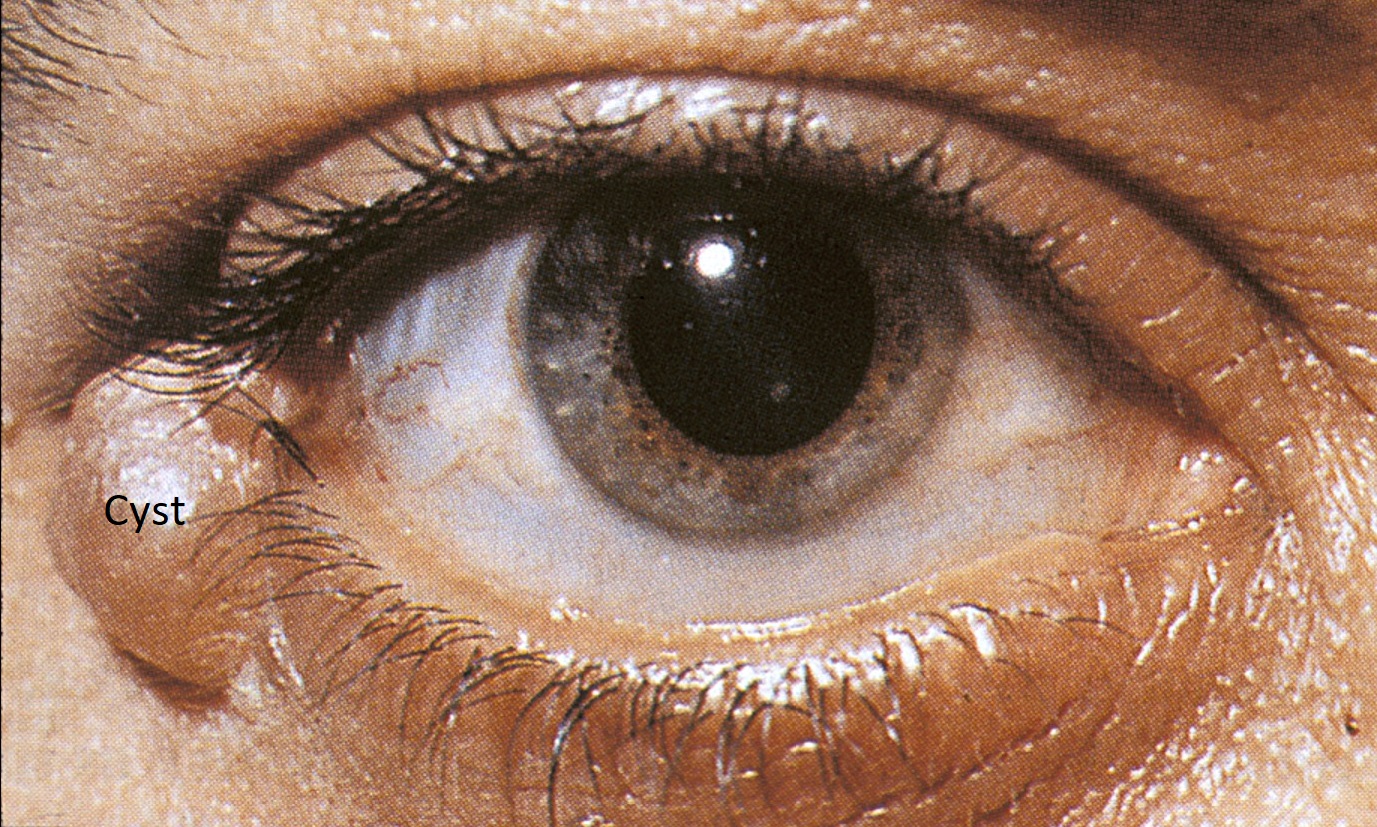
External photo


Eccrine hydrocystoma
- Cystic structure that transilluminates on clinical exam
- More common than apocrine hydrocystoma
- Bilayered cuboidal epithelium lining
- No apices protruding into lumen
Apocrine Hydrocystoma
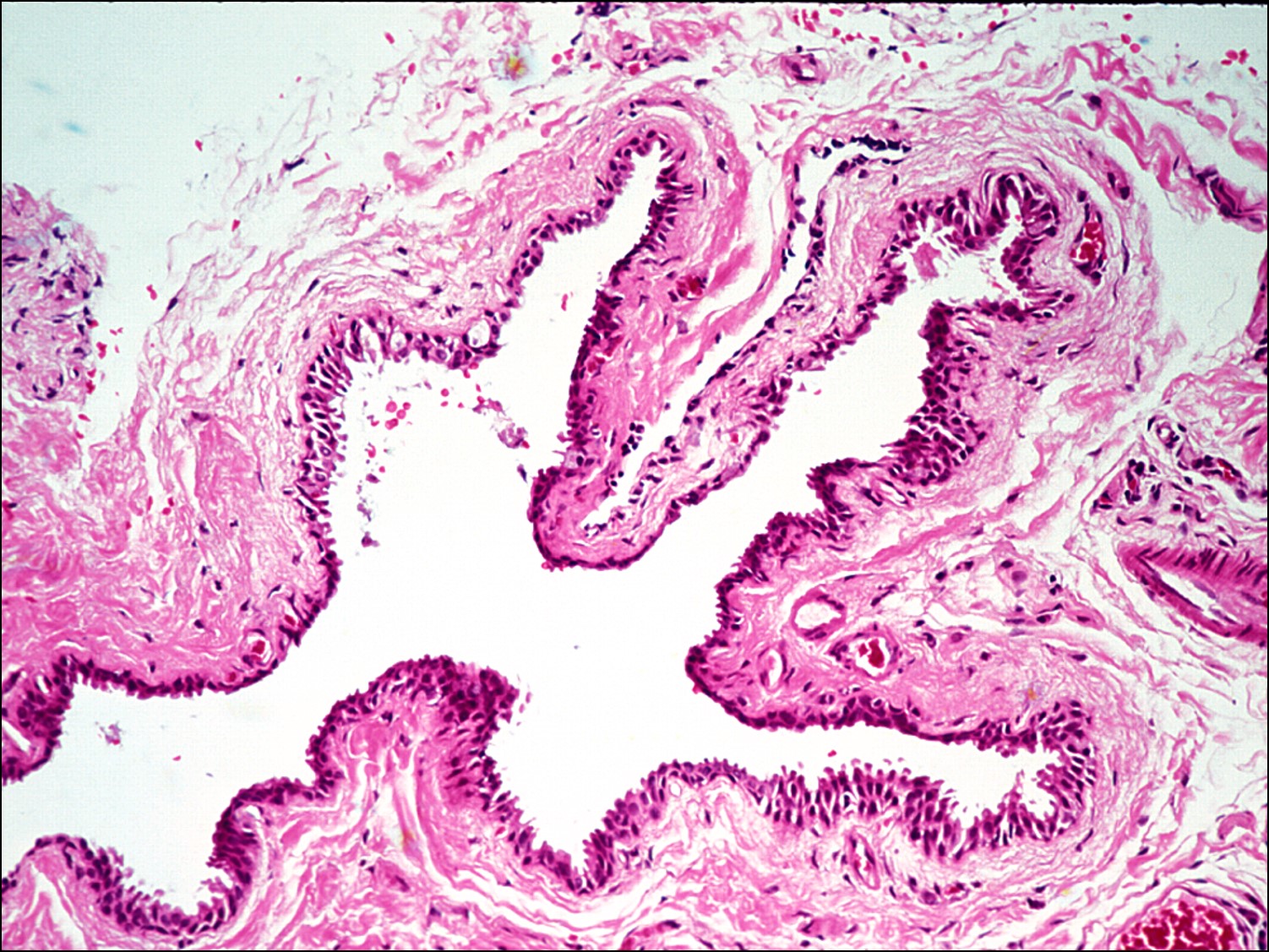

Apocrine hydrocystoma
- Clinical appearance similar to eccrine hydrocystoma
- Bilayered cuboidal epithelium lining
- Apical processes (“snouts”) protrude into lumen
Dacryops
- Cyst arising from lacrimal gland duct
- Thought to be secondary to trachoma, ocular cicatricial pemphigoid, or chemical injury
- Lined by single or bilayered cuboidal epithelium or stratified squamous epithelium with goblet cells and central, fluid-filled lumen
- No cellular atypia
- Surrounding chronic inflammatory infiltrate may be present
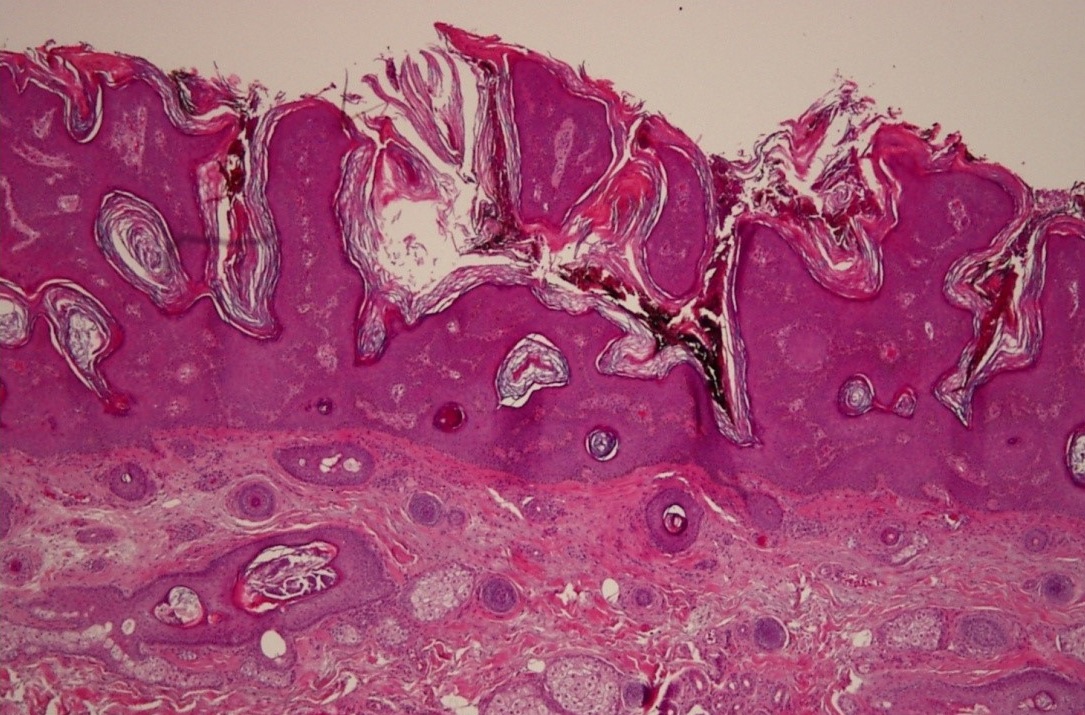
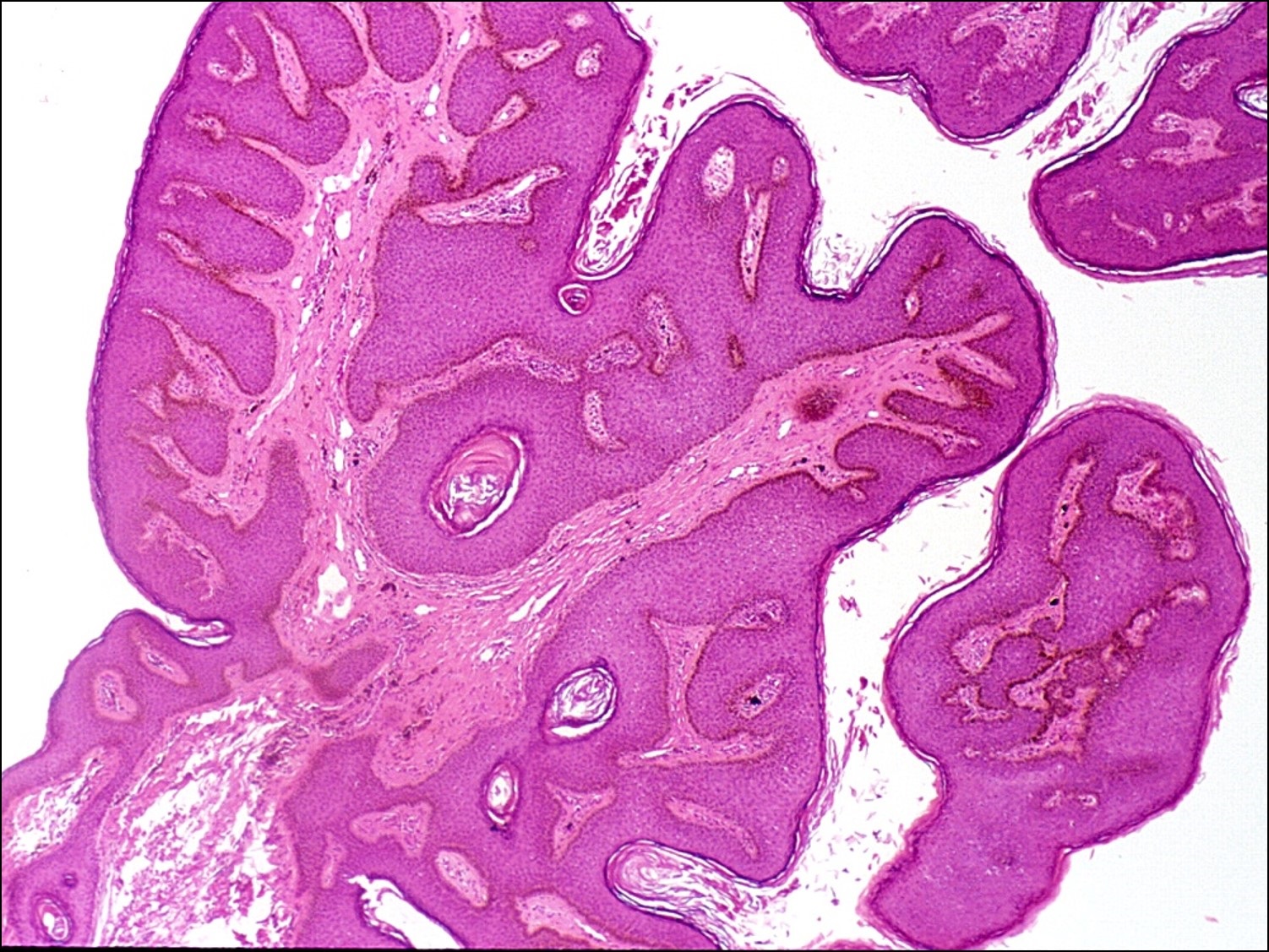
Squamous Papilloma


Squamous papilloma

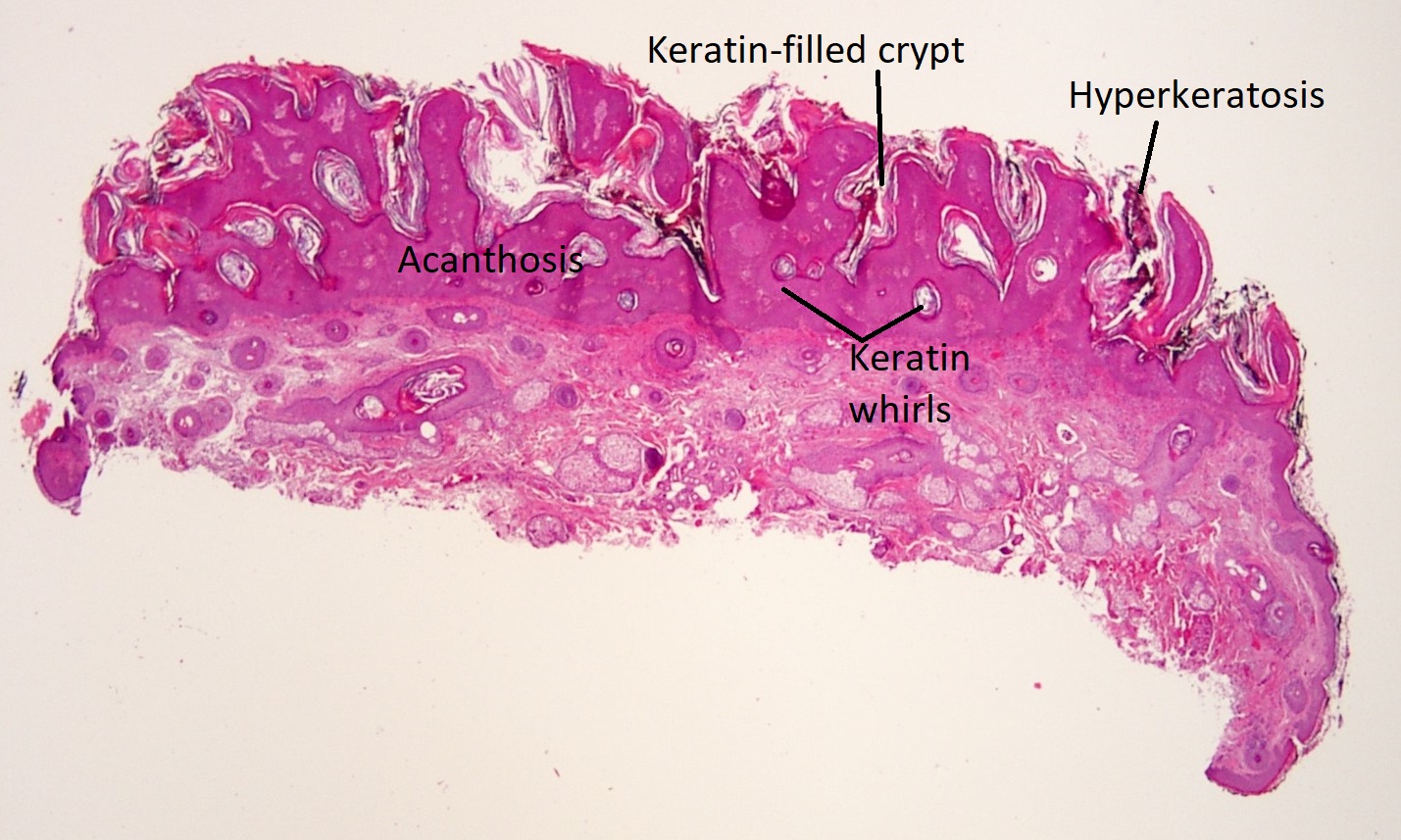
Low magnification

High magnification
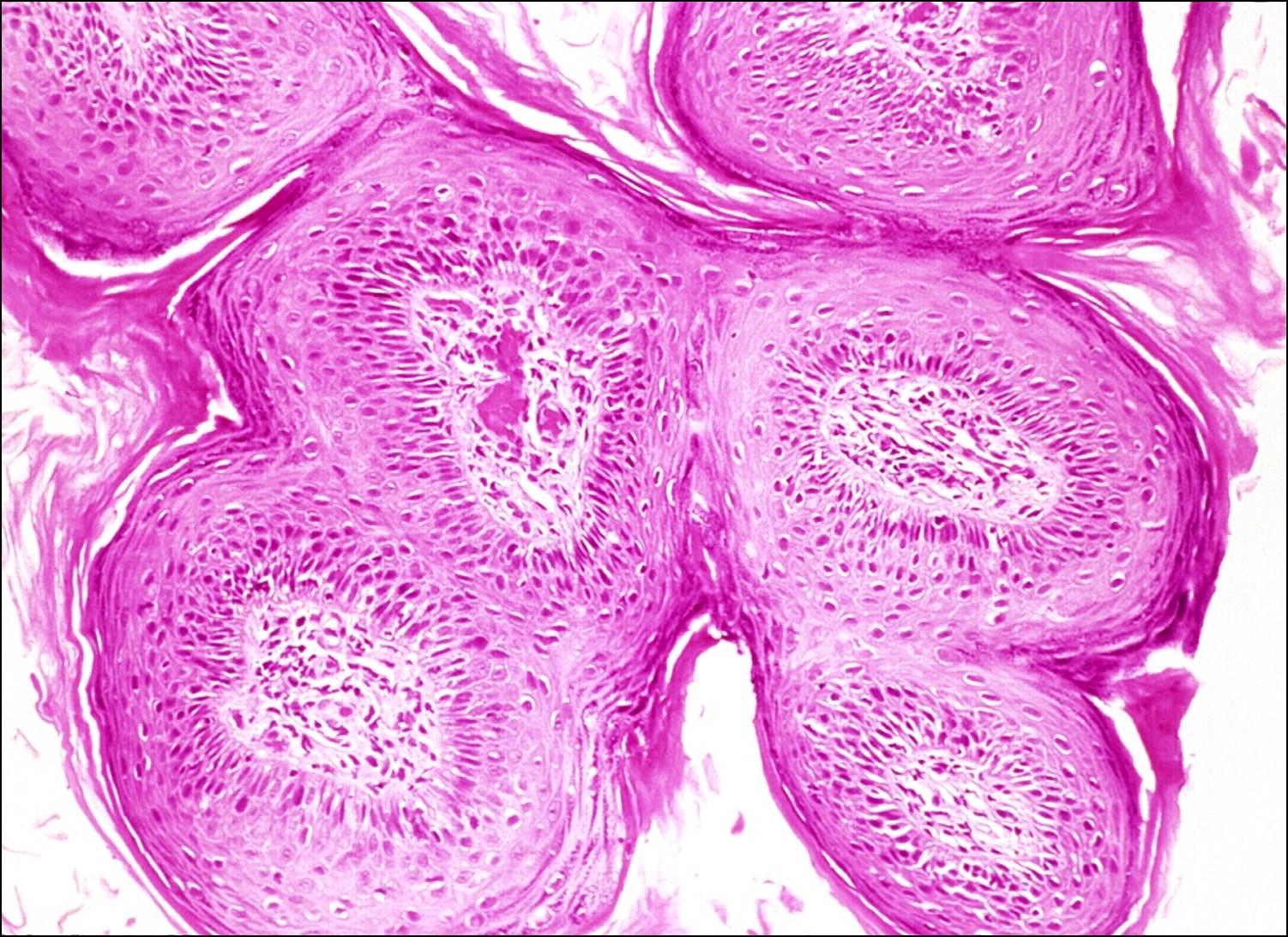
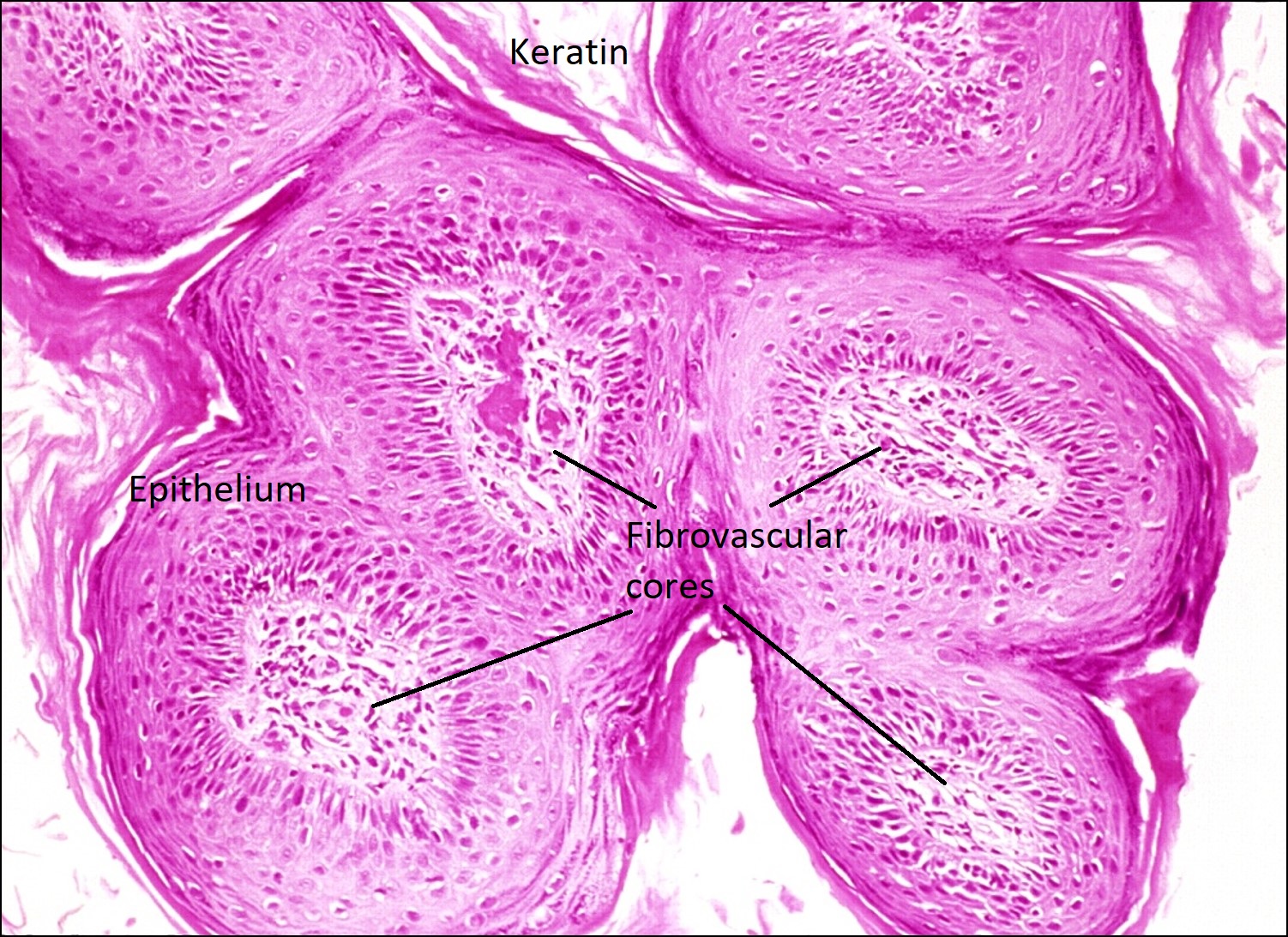
Cross-section of fibrovascular cores
- Most common benign lesion of the eyelid
- Can be sessile or pedunculated
- Acanthotic epithelium with crypts and cysts filled with keratin (hyperkeratosis)
- Papillomatous, fibrovascular cores from the dermis extend into epidermis
- Similar to verruca vulgaris, but without viral inclusions
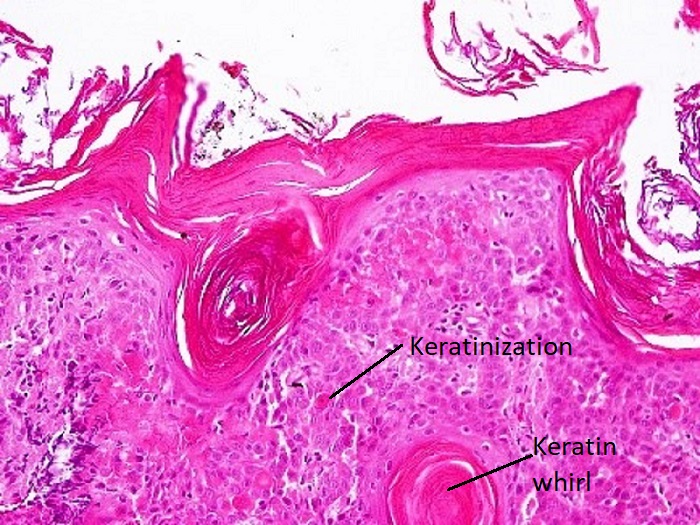
Seborrheic Keratosis


Seborrheic keratosis

Keratin whirls

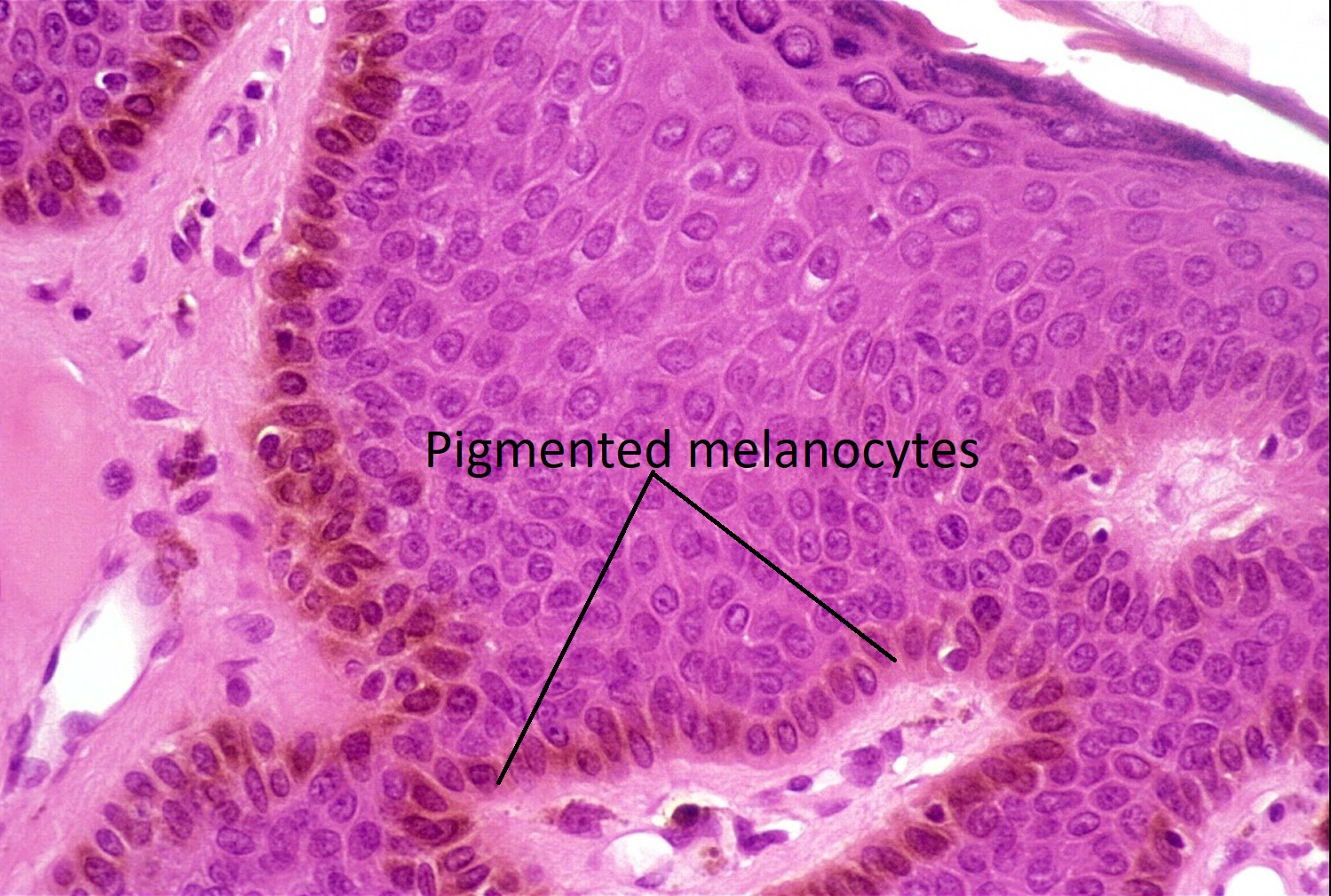
Pigmented melanocytes
- Oily, stuck-on, tan or brown, well-circumscribed lesion commonly found in the elderly
- Common, benign epithelial proliferation
- Hyperkeratosis, acanthosis, papillomatosis, no dysplasia, keratin whorls
- Leser-Trélat sign: sudden onset of multiple seborrheic keratoses, sign of malignancy (GI adenocarcinoma)
Nick’s tips: In seborrheic keratosis, there are finger-like projections of epidermis that go into the dermis, so it takes on more of a “hairy spider” appearance. However, in squamous papilloma, fibrovascular cores project up or out from the dermis into the epidermis, taking on a “gloved hand” morphology.
Trichilemmoma
- Benign neoplasm of cells from the outer hair sheath
- Glycogen-rich cells appear clear on microscopy
- Thickened basement membrane, acanthosis
- Cowden disease: autosomal dominant disease with multiple trichilemmomasand associated with breast, uterine, thyroid, and GI lesions
Keratoacanthoma
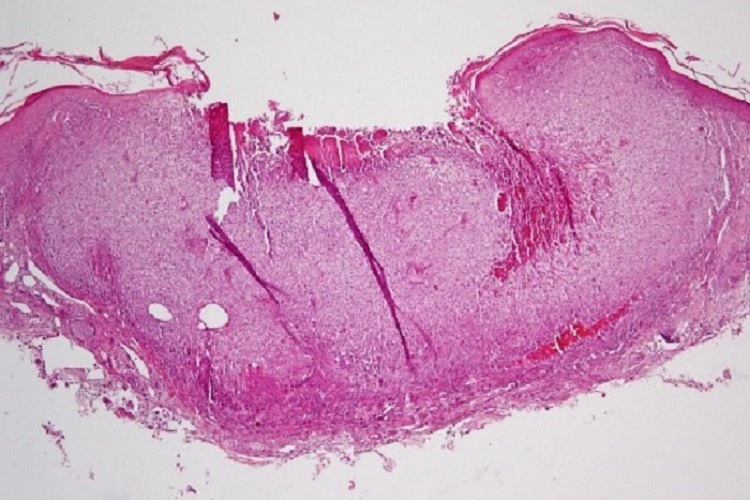
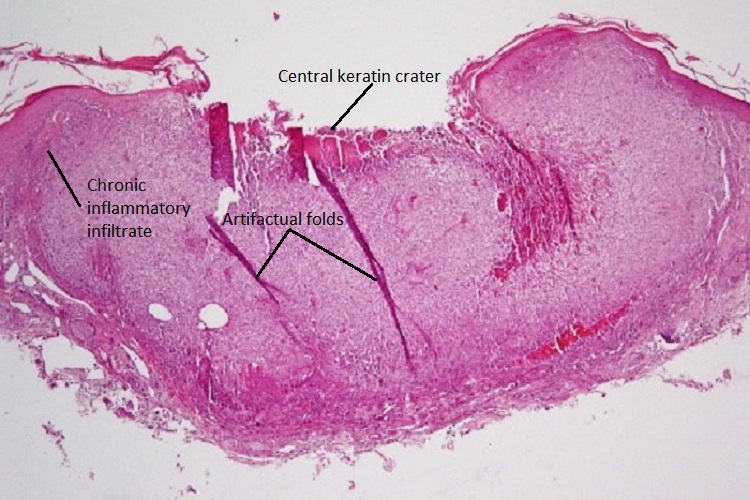
Keratoacanthoma
- Flesh-colored nodule with central keratin crater formed due to rapid epithelial proliferation
- Areas of well-differentiated squamous epithelium surround a central keratin mass
- Chronic inflammatory infiltrate (lymphocytes and plasma cells) at base of lesion
- Atypical cells may be present at the deep border of the lesion
- Variant of well-differentiated squamous cell carcinoma with low malignant potential
- Usually spontaneously involutes, leaving behind a slightly depressed scar
Actinic Keratosis
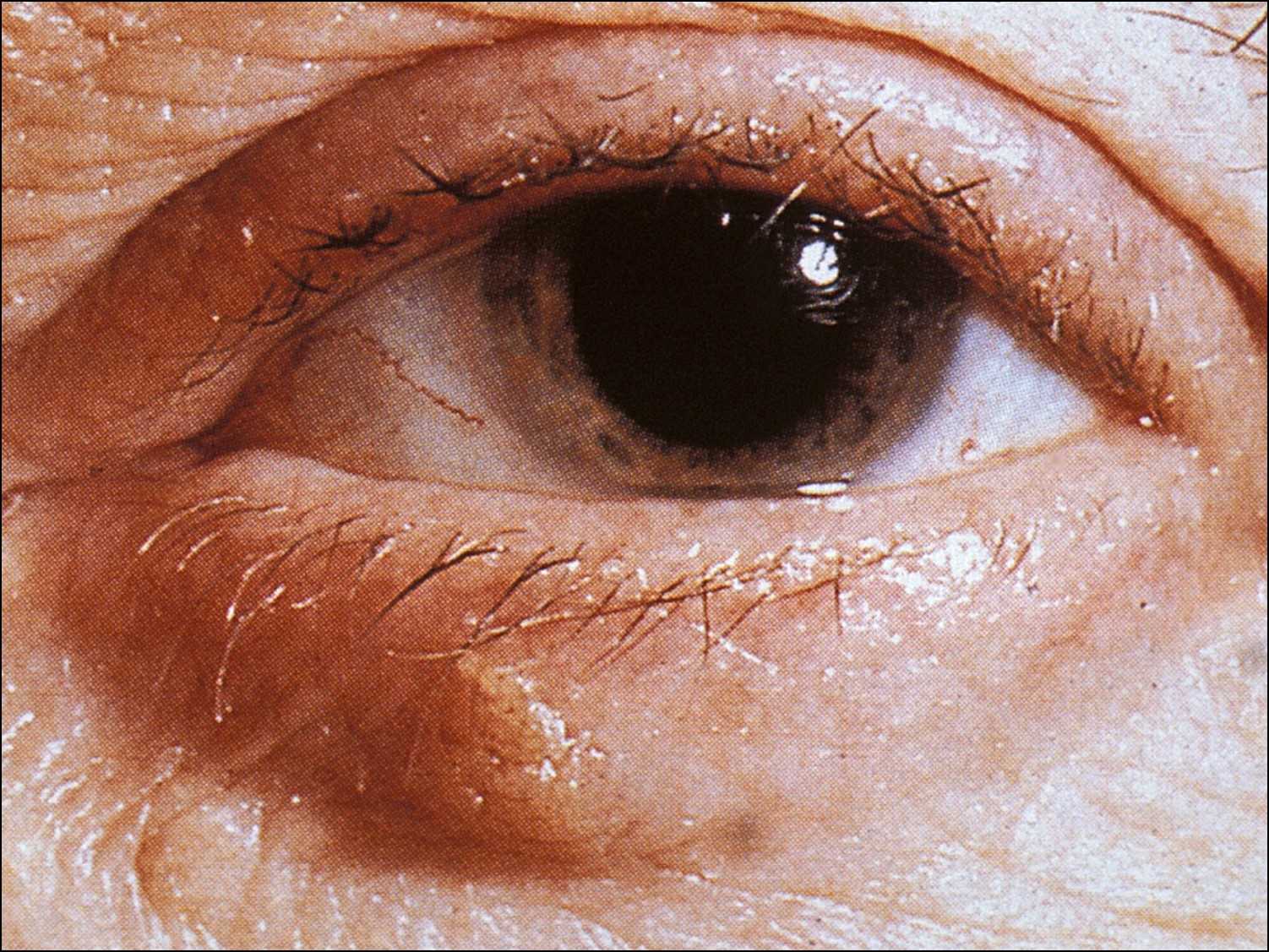

Actinic keratosis
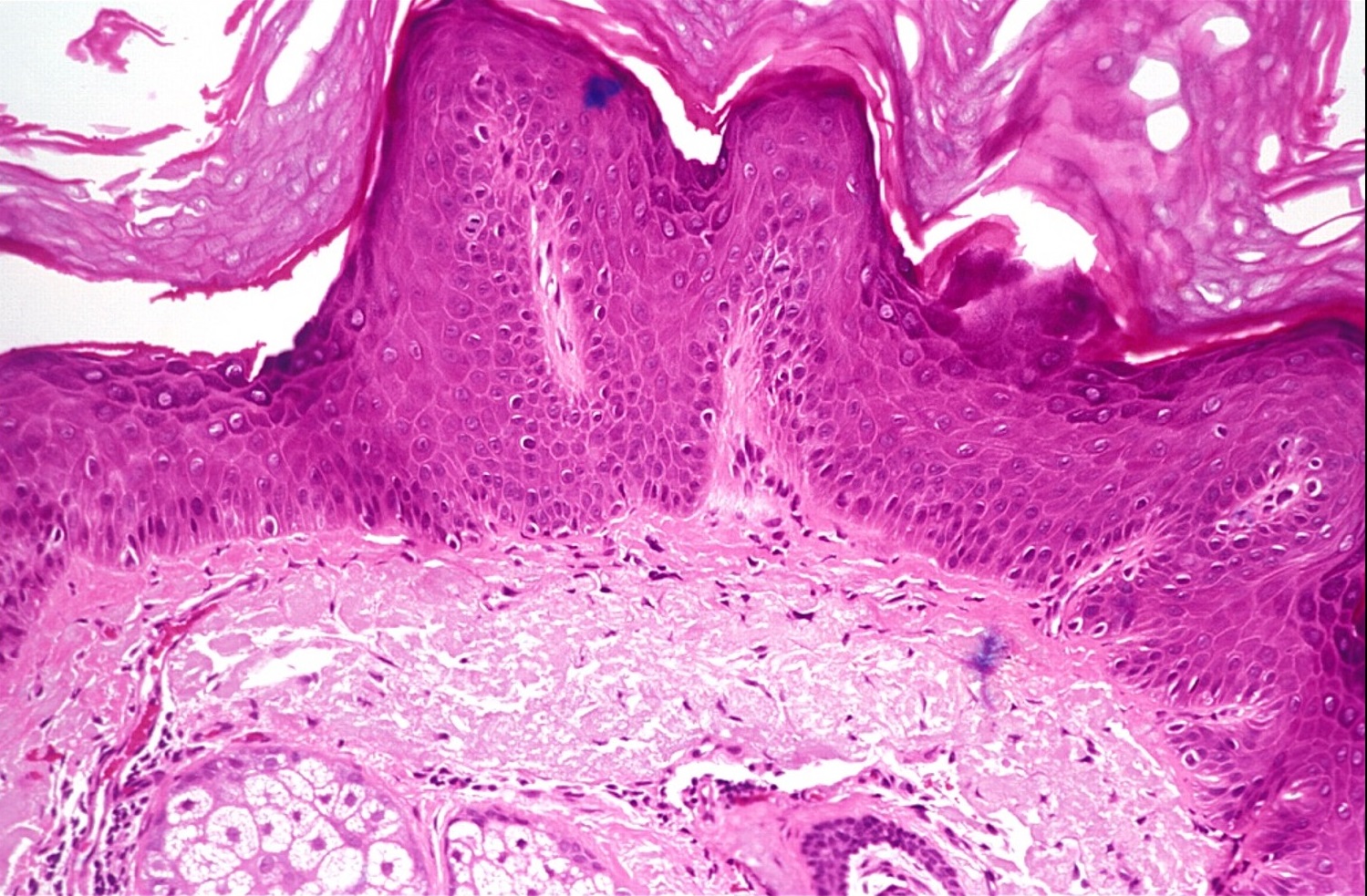
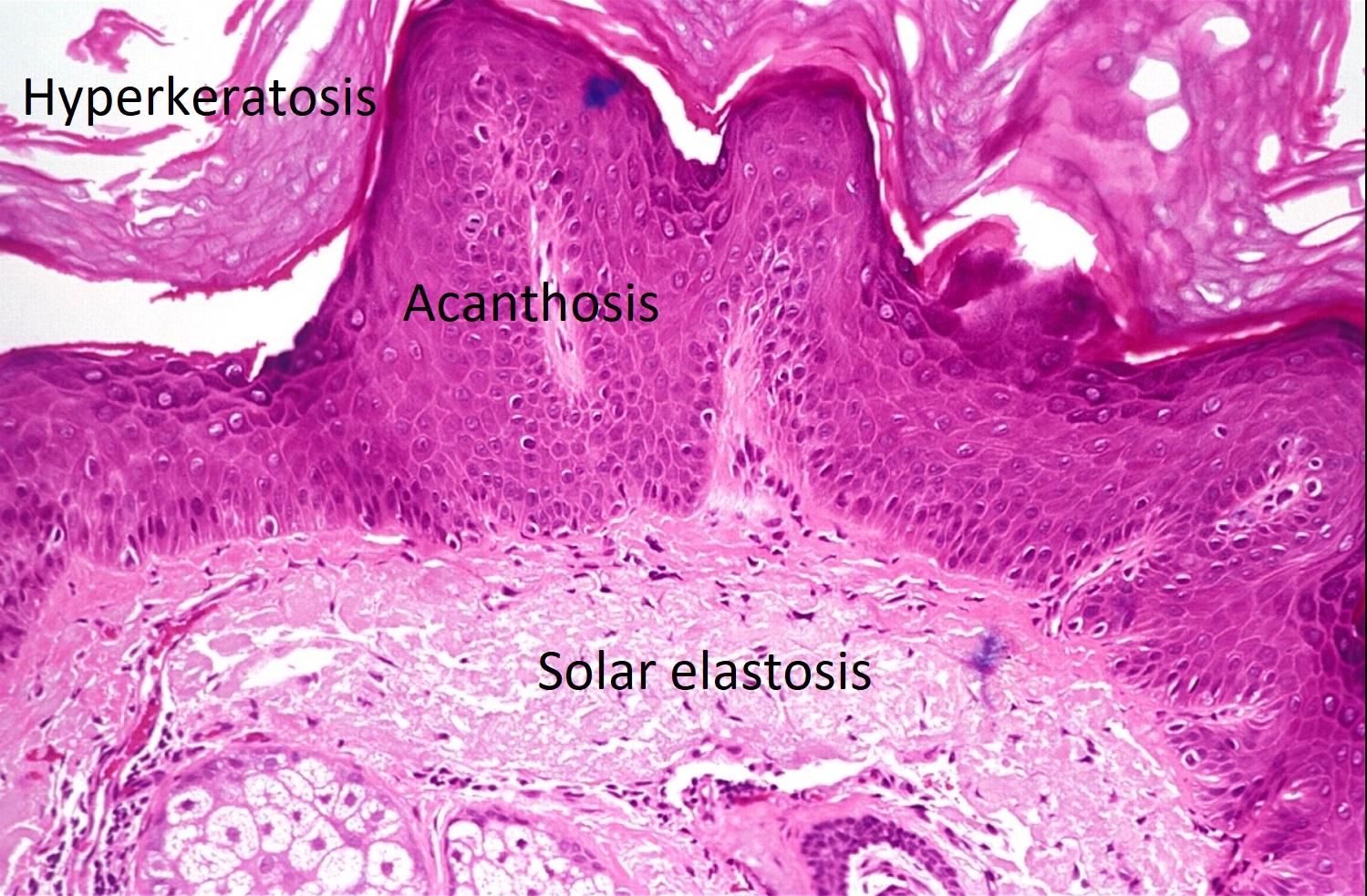
Solar elastosis
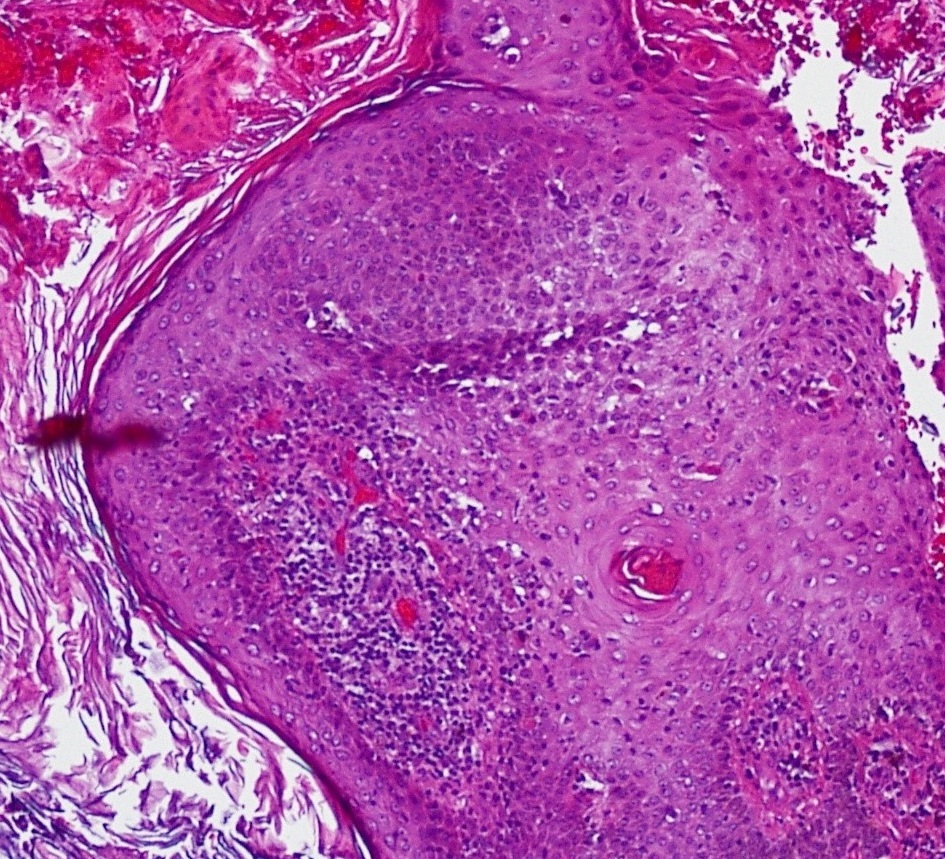

Keratin whirls and atypia
- Also has scaly, pigmented appearance similar to seborrheic keratosis
- Due to solar exposure, so commonly found on sun-exposed areas
- Most common precancerous cutaneous lesion
- Can become a malignant squamous cell carcinoma
- Epithelial findings: Solar or senile keratosis, acanthosis, hyperkeratosis, parakeratosis, atypical epithelium with nucleoli present
- Dyskeratosis: indicates likelihood of becoming malignant
- Dermal findings: solar elastosis, basophilic degeneration of collagen, chronic inflammatory infiltrate (lymphocytes and plasma cells)in superficial dermis
Nick’s tips: Since the basement membrane in actinic keratosis is still intact, it is essentially like carcinoma in situ of the eyelid. Make sure to include the base of the lesion in the biopsy so an invasive squamous cell carcinoma can be ruled out.
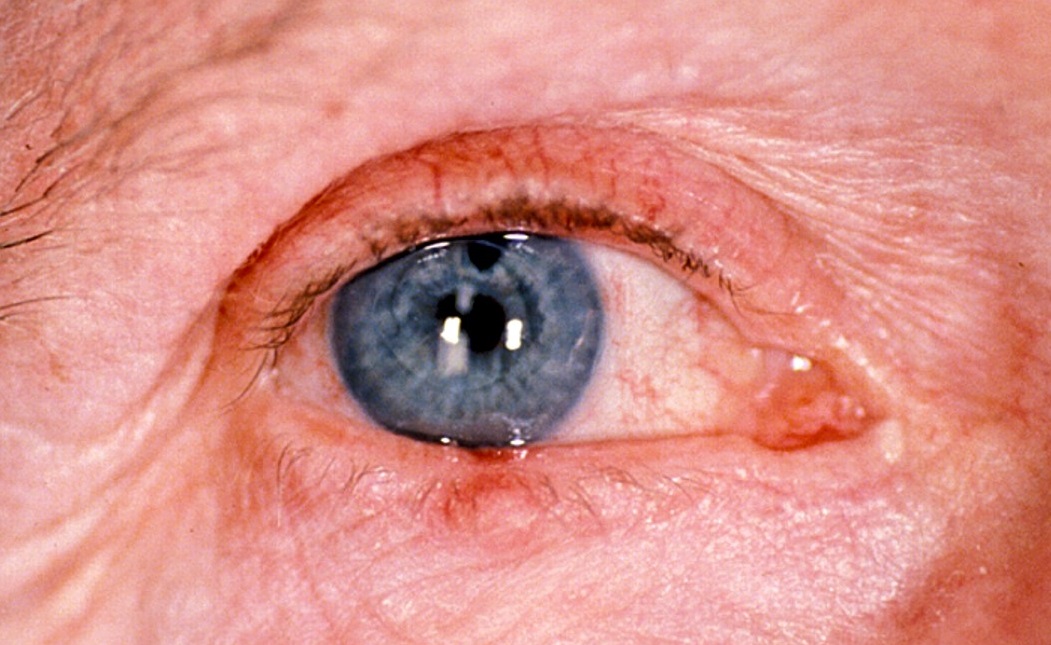
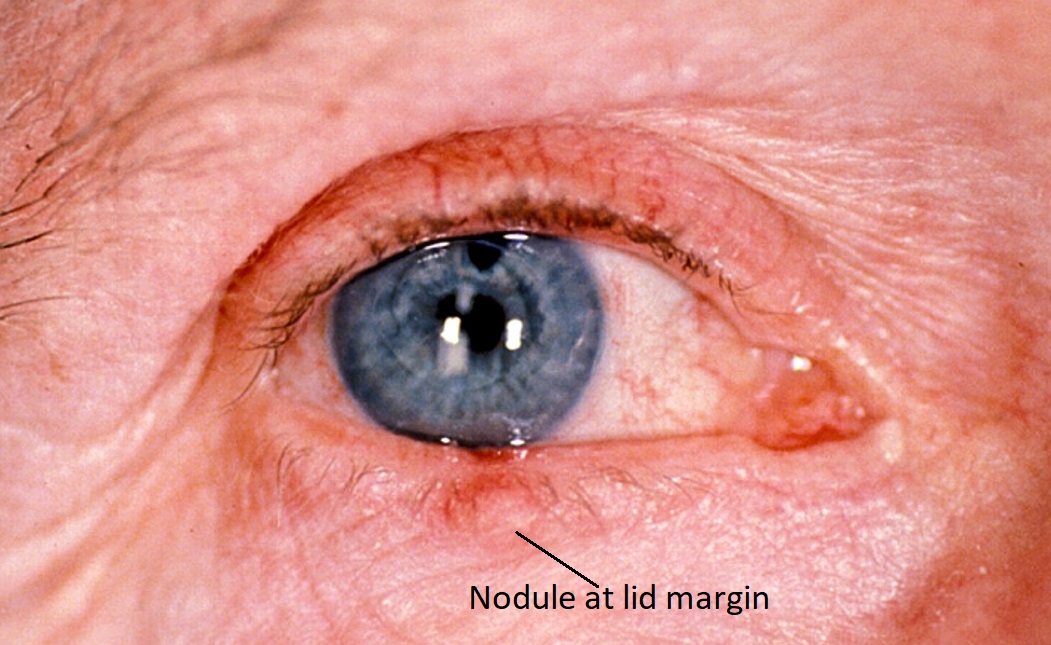
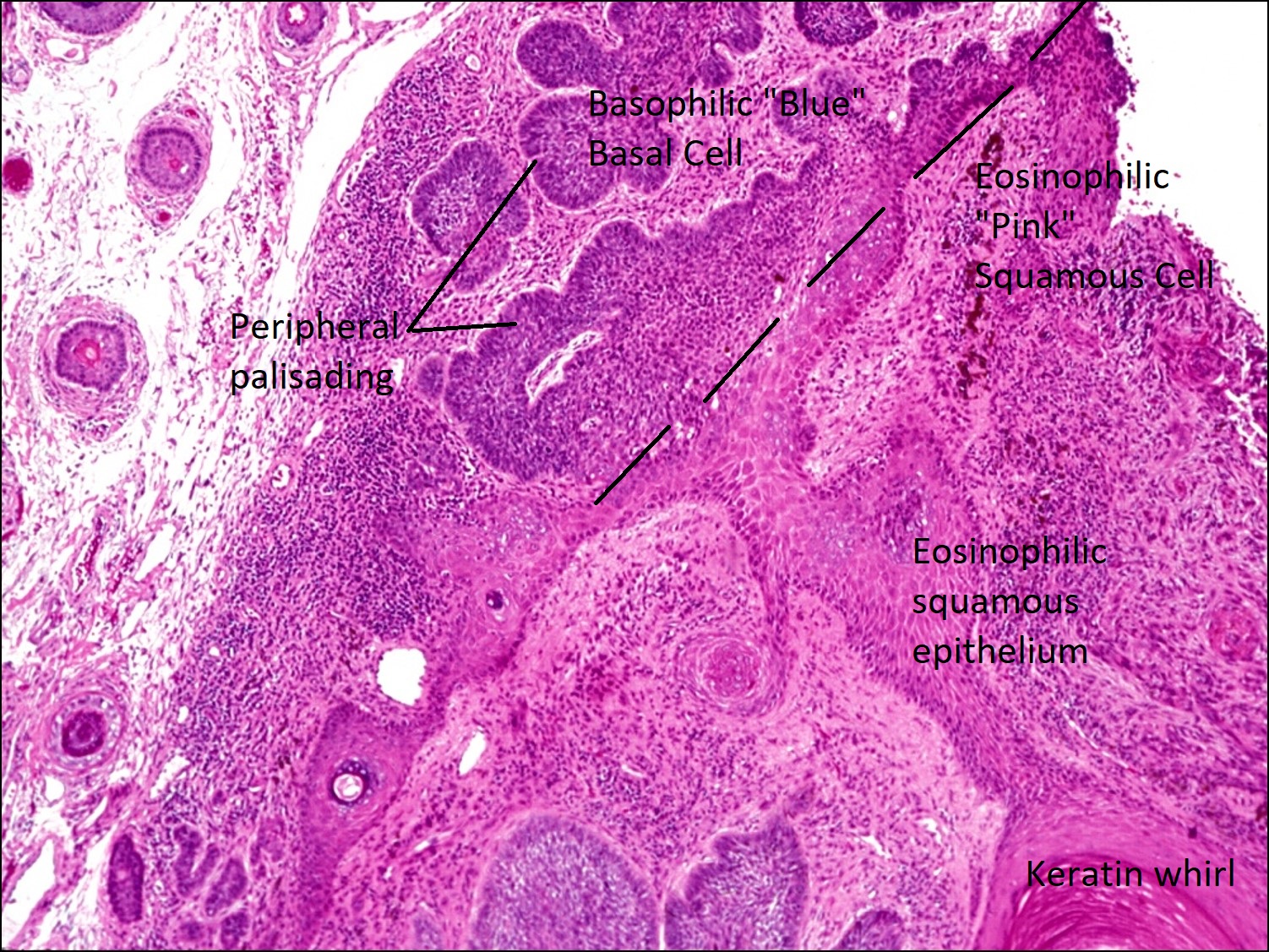
Basal Cell Carcinoma (BCC)


Ulcerated BCC

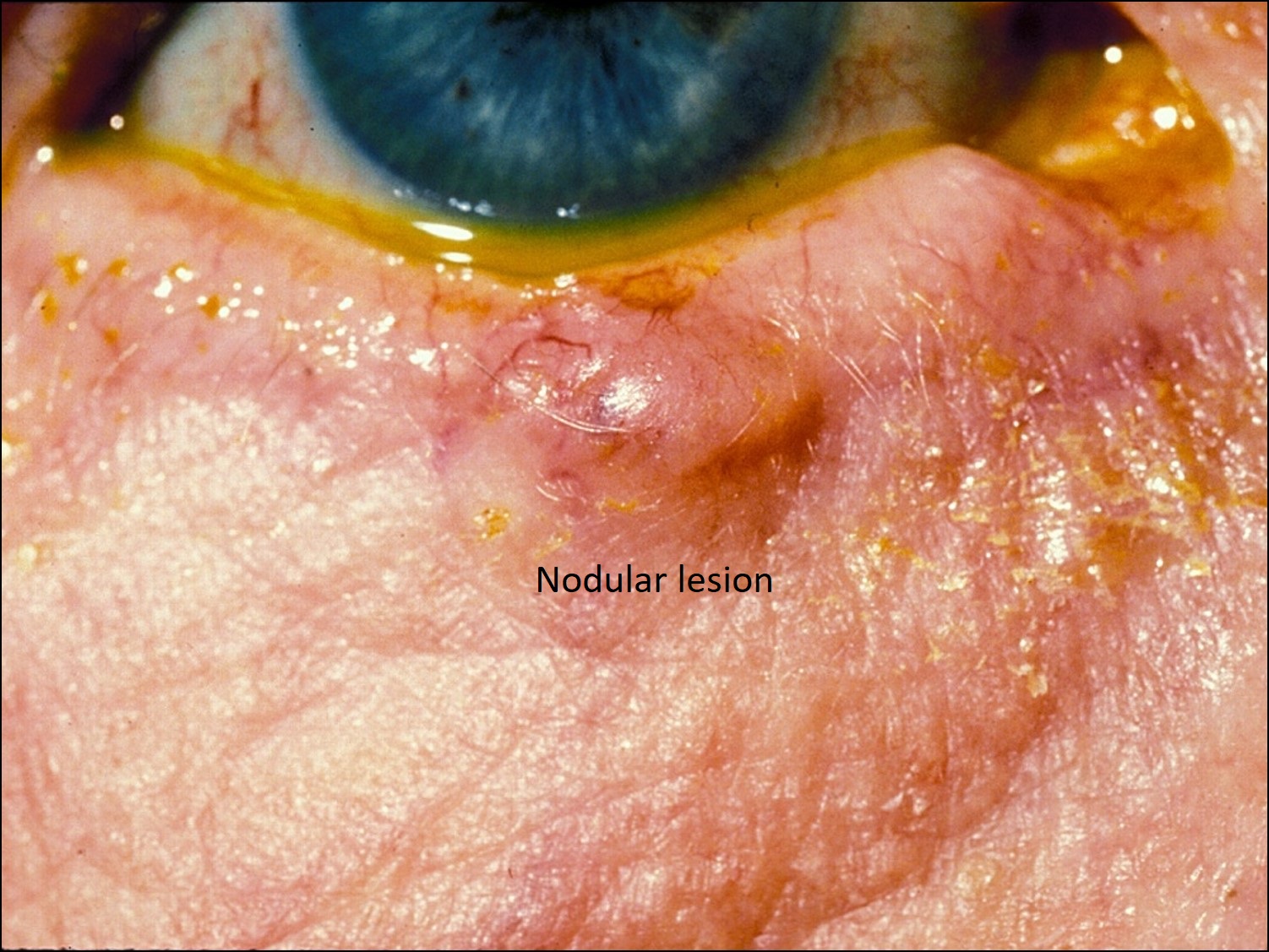
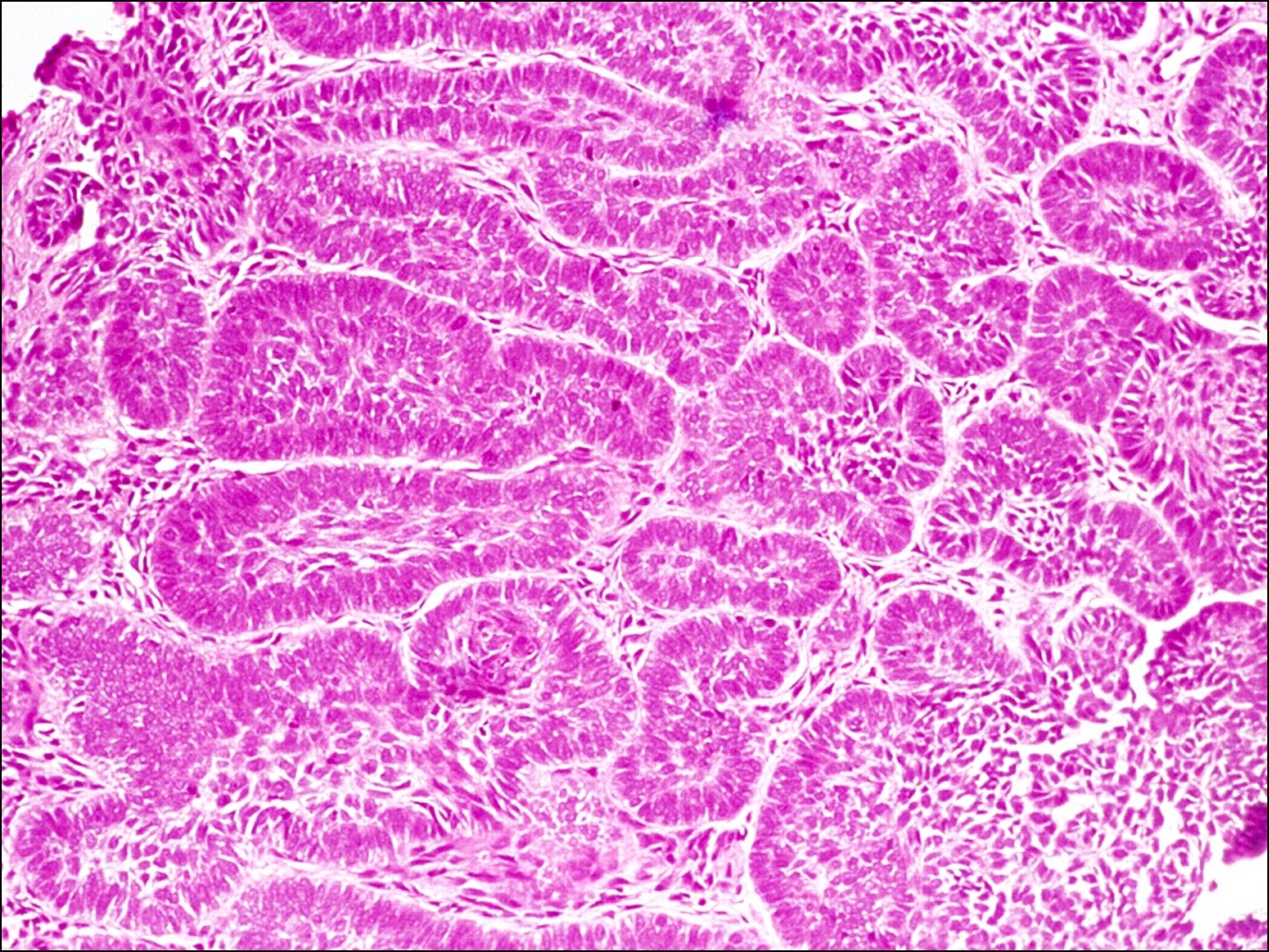
Nodular BCC

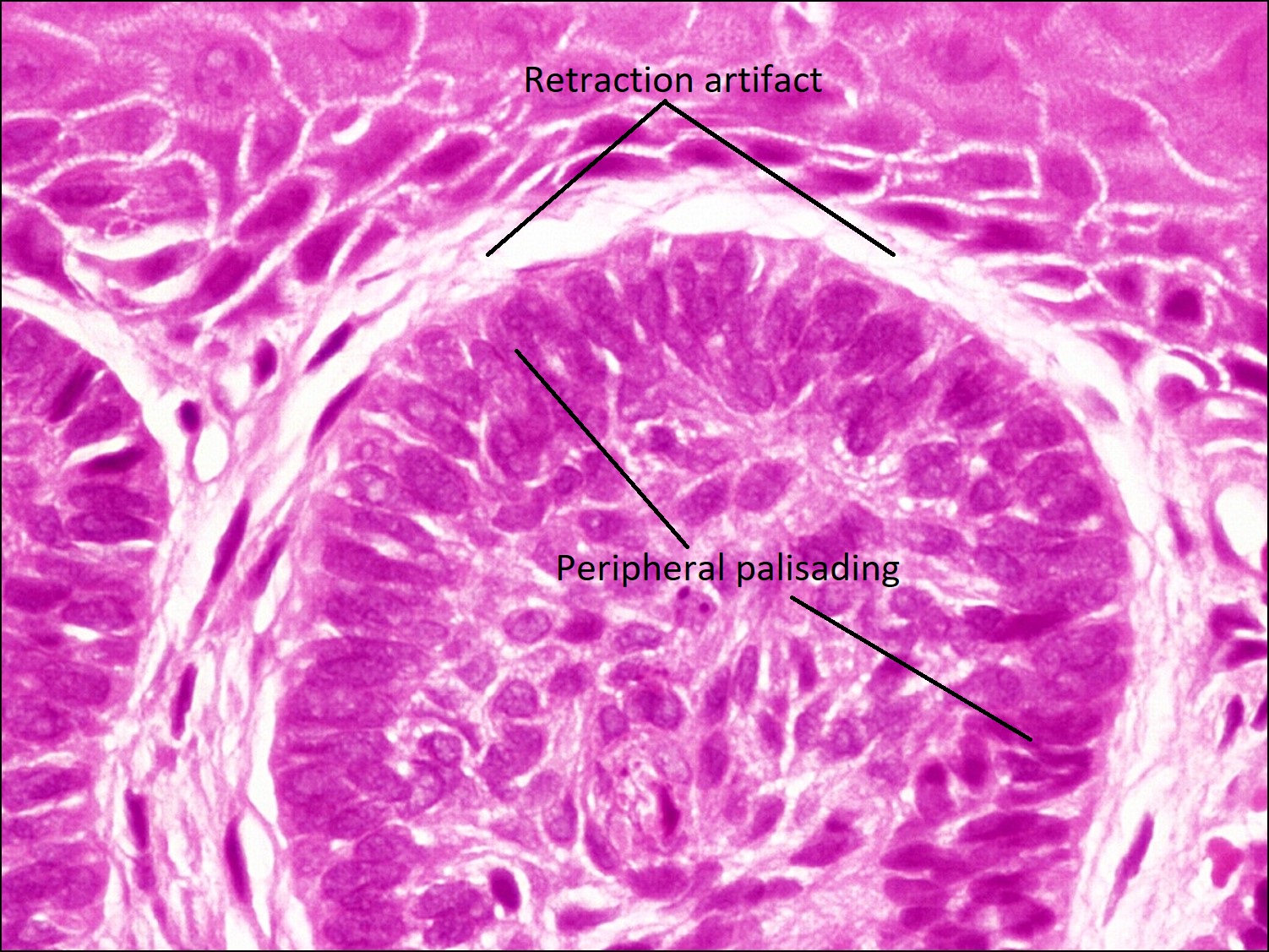
Peripheral palisading

High magnification


Nodulocystic BCC

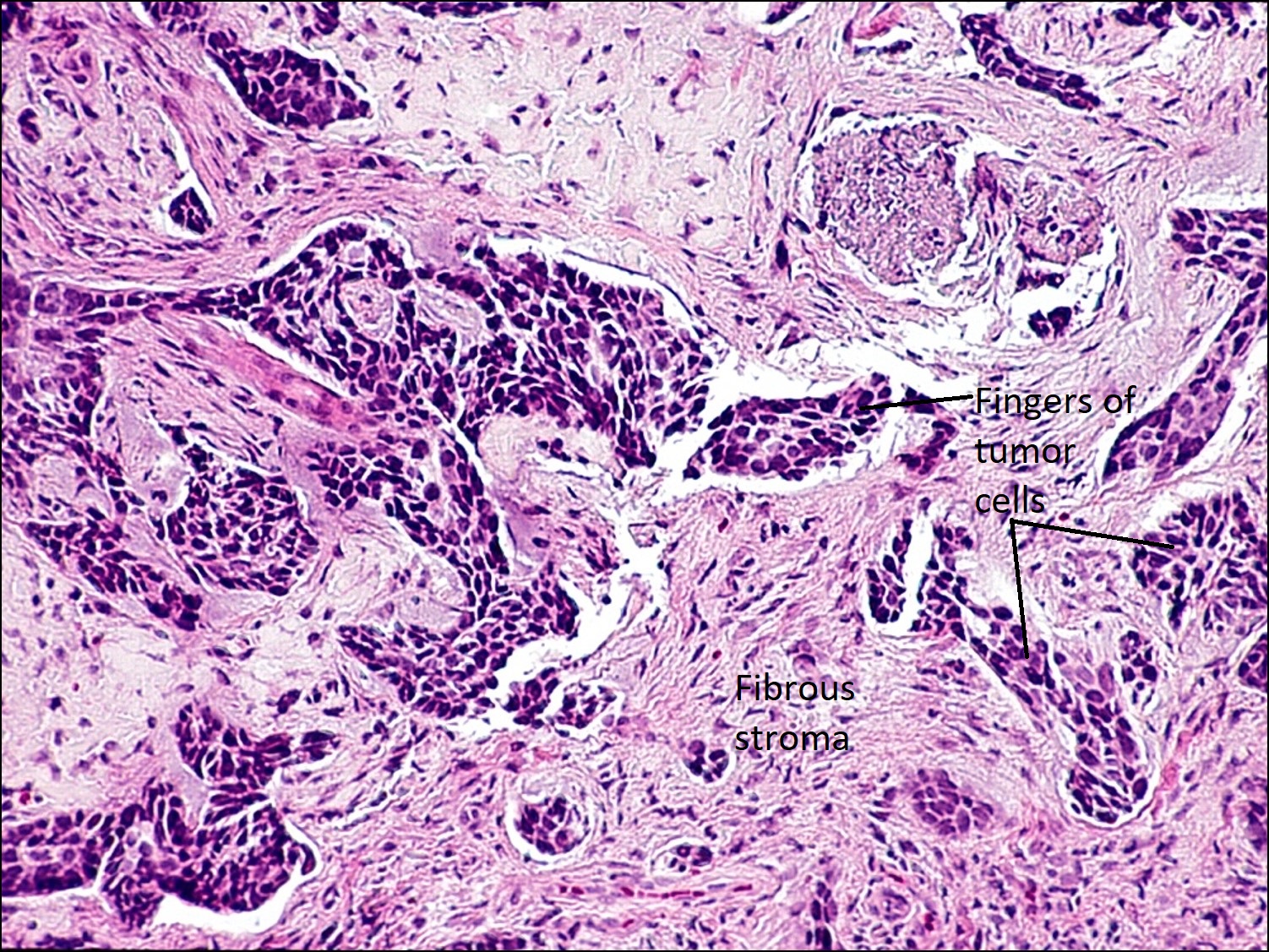
Morpheaform BCC

Basosquamous BCC

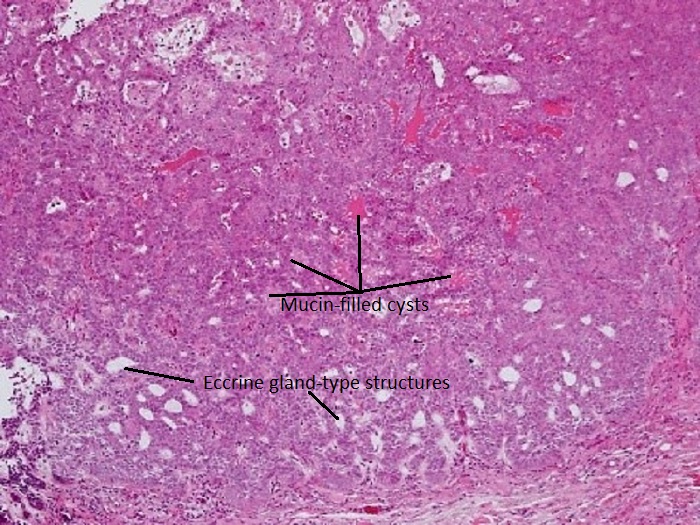
Differentiated Adenoid BCC
- Most common malignant tumor of the eyelid, 40 times more common than SCC
- Most common location: lower lid
- Second most common location: medial canthus (more likely to involve orbit and be deeply invasive)
- Unlikely to occur on upper lid because the brow shades the upper lid
- Elevated nodule with pearly, raised edges and central ulceration
- Can also appear as a flat yellowish indurated plaque (morpheaform type)
- Causes: sun exposure, some genetic component in familial syndromes
- Characteristic islands of tumor cells with peripheral palisading of nuclei and a meaningful artifact of tumor shrinkage from surrounding tissue
- Differentiated types: pluripotent cells differentiate into skin and skin appendage-like structureso
- Keratotic –hair
- Cystic –sebaceous glands
- Adenoid –apocrine & eccrine glands, cystic spaces filled with mucin
- Undifferentiated types:
- Nodular: lobules of tumor cells with pseudocapsule (retraction artifact)
- Contents can be solid or cystic
- Nodular cystic BCC: nodular type with large areas of necrosis
- Mostcommon type of BCC
- Ulcerative: present with surrounding chronic inflammatory infiltrate in the dermis
- Morpheaform: fingers or “Indian filing” of tumor cells with surrounding fibrous stroma
- More aggressive form of BCC with a worse prognosis
- More difficult to know if fully excised
- Multicentric: epidermis and superficial dermis diffusely involved
- Basosquamous: morphology between BCC and SCC and more aggressive type
- Nodular: lobules of tumor cells with pseudocapsule (retraction artifact)
- Treatment: complete excision
- Mohs surgery essential for Ulcerative, Morpheaform, and Multicentric types
- Prognosis
- Morbidity relates to local spread
- Metastasis extremely rare
Squamous Cell Carcinoma(SCC)


Nodule of SCC


Diffuse SCC lesion
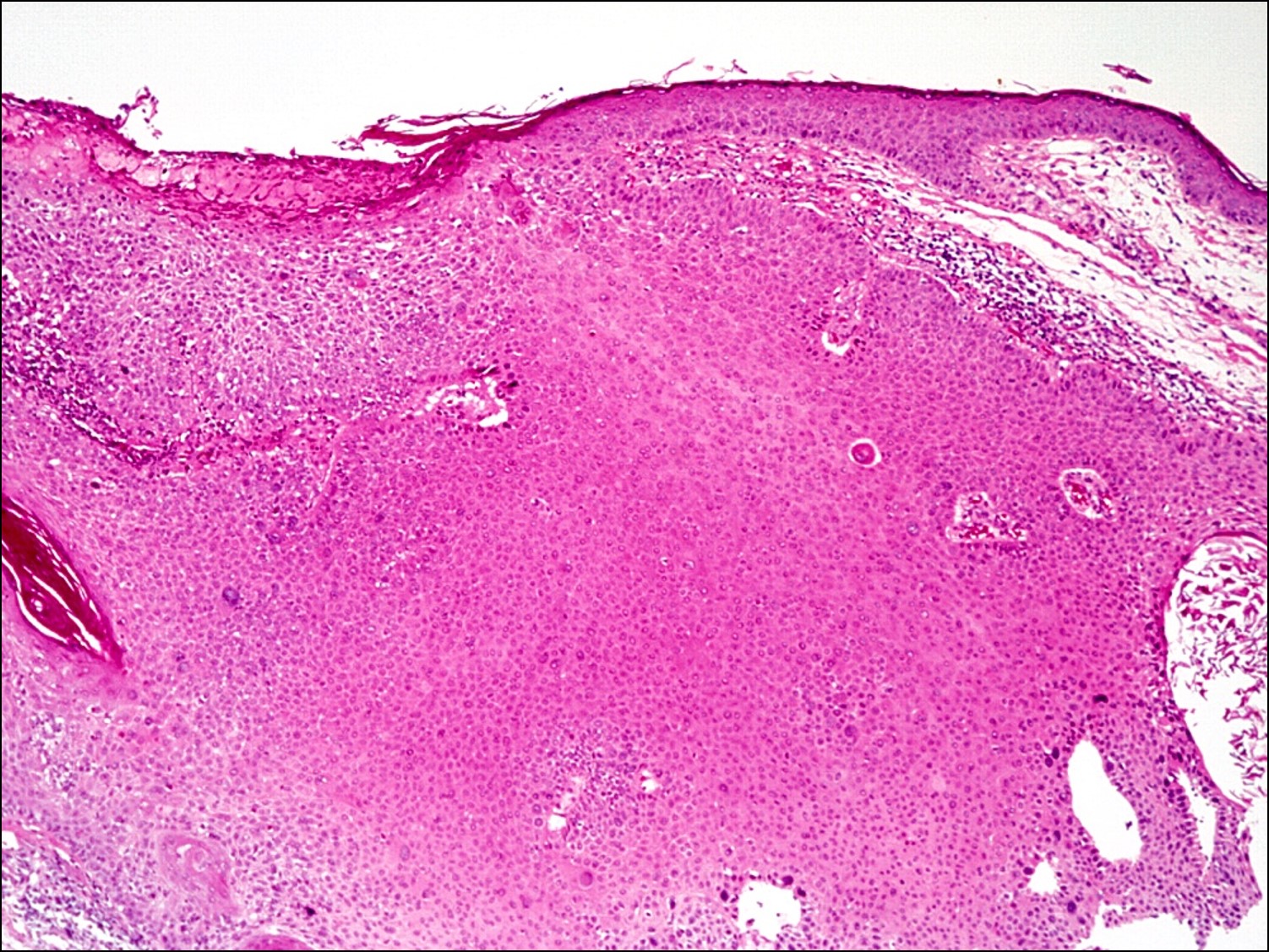

Squamous cell carcinoma
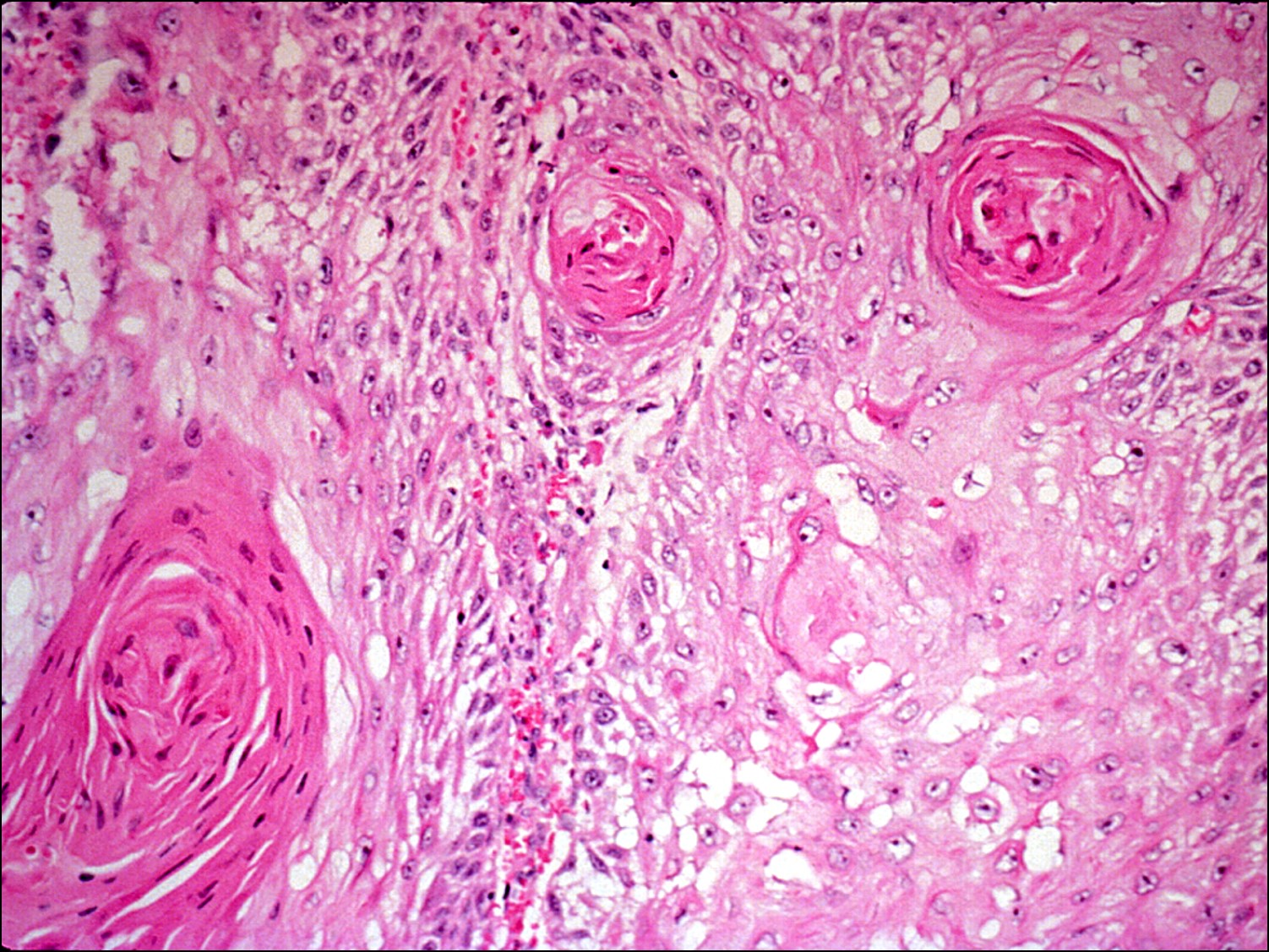

Higher magnification
- Second most common malignancy of the eyelids
- Most commonly arise from actinic keratosis and sun damaged skin
- More likely to involve the lower lid than the upper lidHowever, of upper eyelid malignancies, SCC is more likely than BCC.
- Clinical appearance can vary from ulcers to plaques and nodular to fungating
- Typical presents as a scalyorange plaque or nodule with parchment paper-like skin, madarosis (lash loss), and surrounding sun-damaged skin that may be ulcerated
- Nests or strands of atypical squamous cells invading the basement membrane and dermis
- Well-differentiated: keratin whirls, intercellular bridges, dyskeratosis, acanthosis
- Spindle cell variant: appears like fibrous histiocytoma or fibrosarcoma
- Adenoid variant: pseudoglandular structures from atypical cuboidal epithelium
- Uncommonly affects eyelid
- Good prognosis
- Treatment: wide local excision
- Prognosis
- Perineural or lymphatic invasion worsens prognosis
- Mohs surgery is indicated
- Up to 20% experience metastasis to a regional lymph node
- Perineural or lymphatic invasion worsens prognosis
Nick’s tips: When in doubt, a basal cell carcinoma is predominantly blue, whereas a squamous cell carcinoma will predominantly stain pink due to the presence of keratin.
Sebaceous Hyperplasia

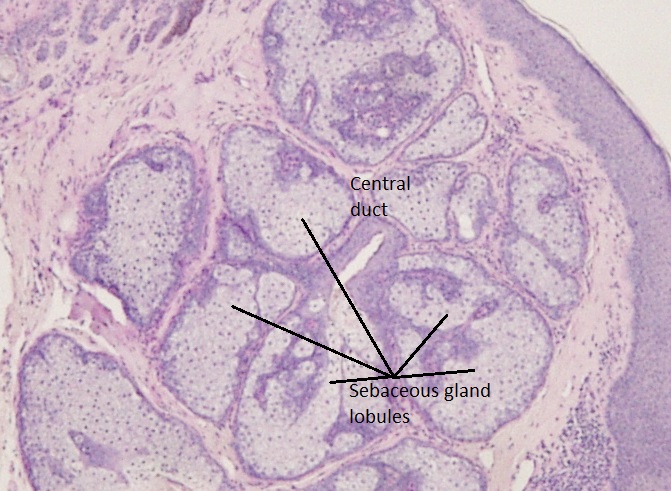
Sebaceous hyperplasia
- Uncommon benign lesion
- Small yellow papule on the face and eyelid
- Several sebaceous gland lobules surrounding a single central duct
- Normal basal layer
Sebaceous Adenoma


Sebaceous adenoma
- Rare benign eyelid lesion
- Firm, yellow, circumscribed nodule
- Multiple incompletely differentiated and irregularly shaped sebaceous lobules
- Localized proliferation of basal basophilic sebocytes
- Undifferentiated, mature, and transitional sebaceous cells present
- Most commonly associated with Muir-Torre syndrome: indication of visceral malignancy (colorectal carcinoma, genitourinary, breast)
Sebaceous Carcinoma
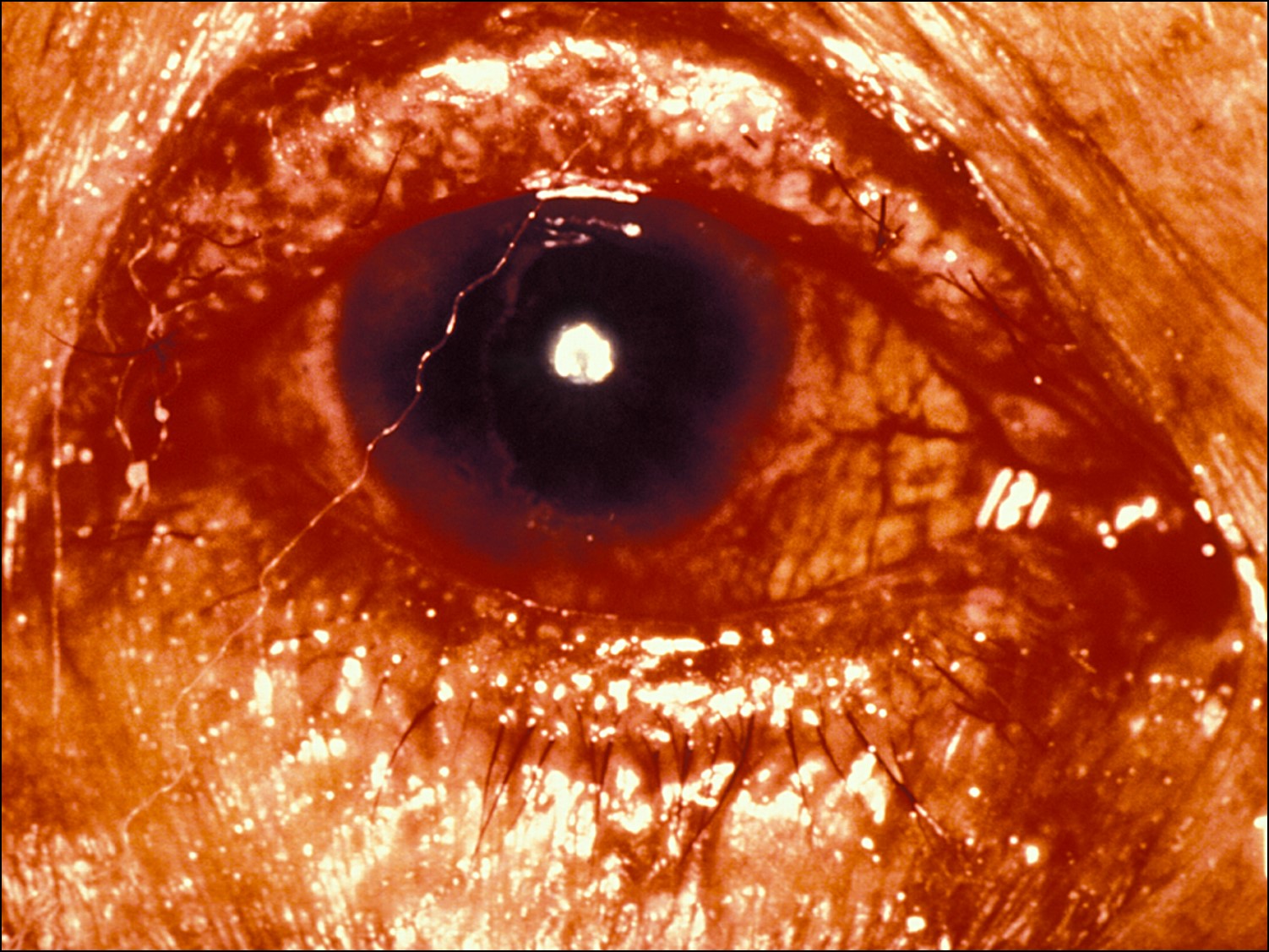
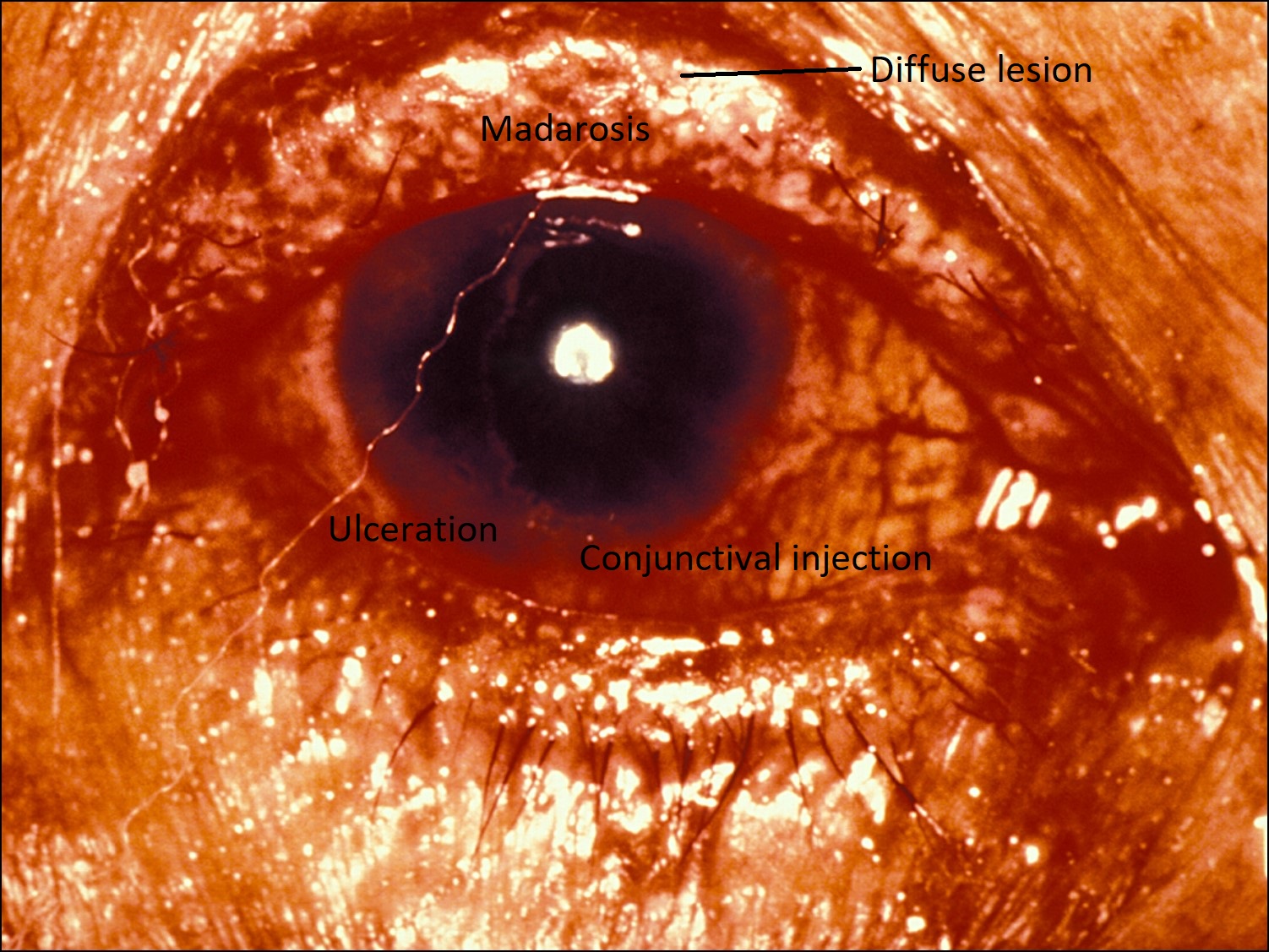
Diffuse Sebaceous carcinoma


Focal sebaceous carcinoma
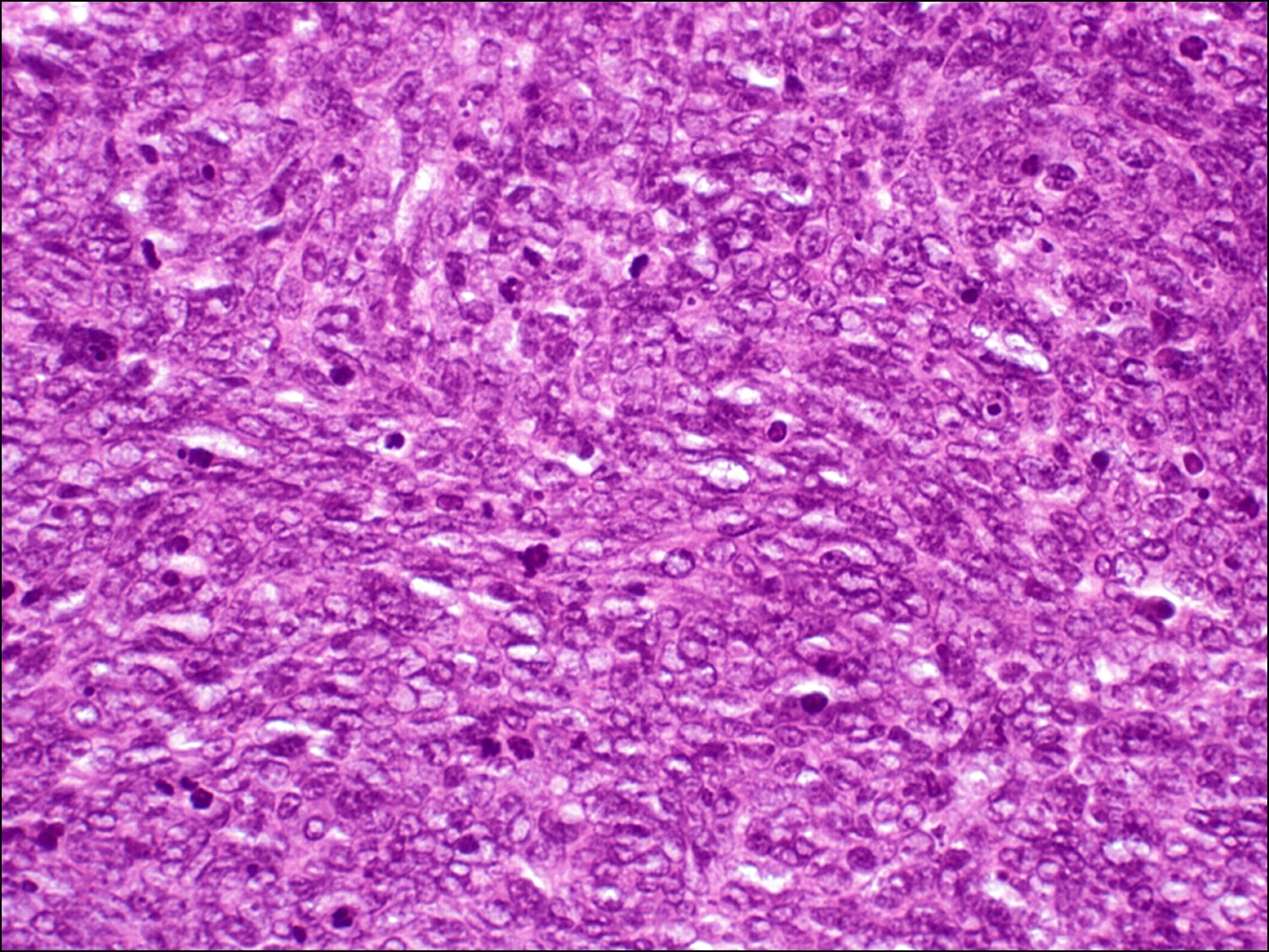

Low magnification

High magnification with mitotic figures
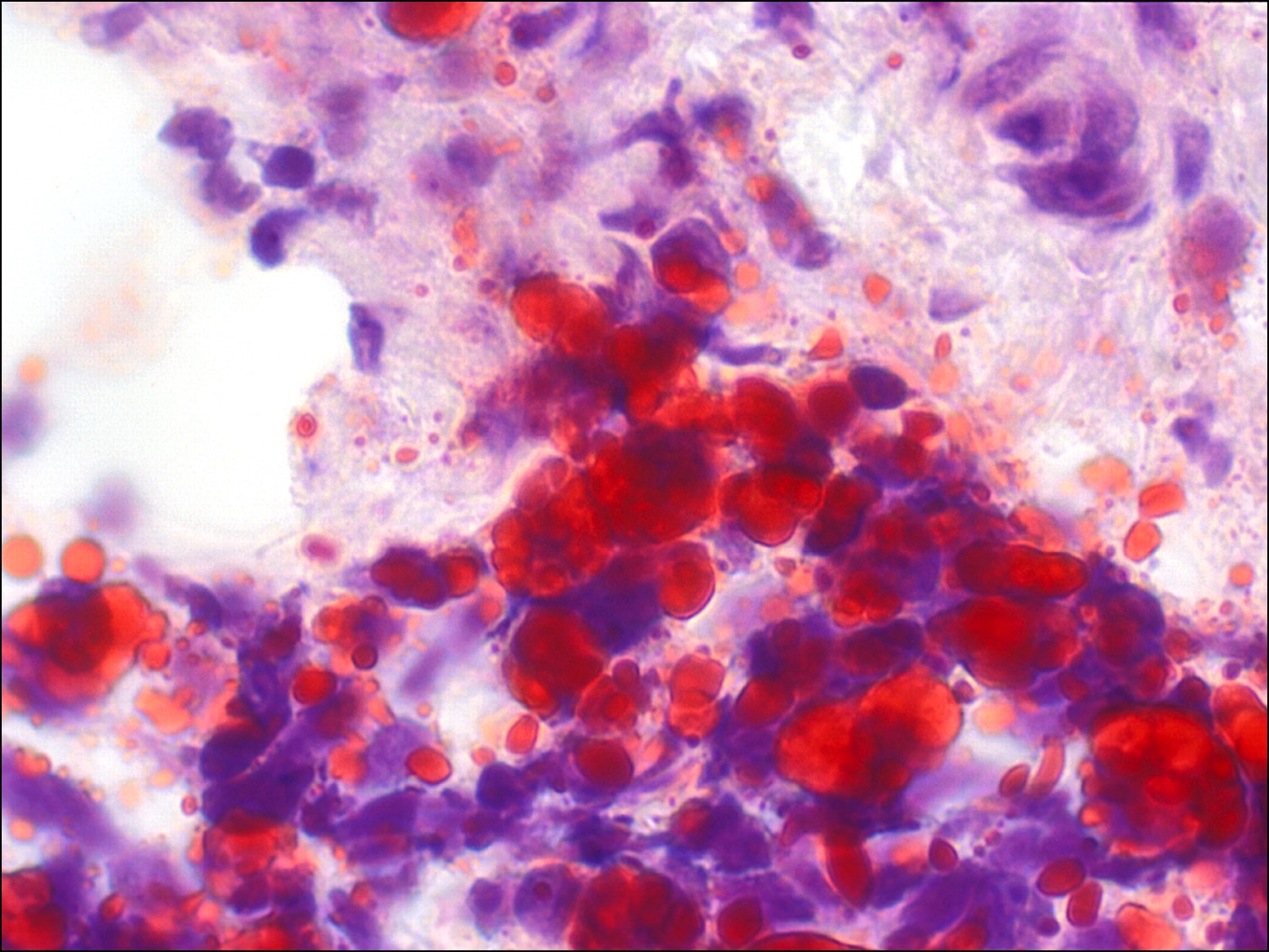

Oil Red O stain
- A yellow-white lesion that can be diffuse or focal, sometimes with diffuse ulceration, conjunctival injection, or madarosis (lash loss)
- Arise from sebaceous glands (meibomian, glands of Zeiss, in the caruncle)
- Aggressive tumor that can metastasize; worse survival rates than squamous cell carcinoma
- Most commonly involves the upper lid because it has twice the number of meibomian glands
- Tumor cells with mitotic figures
- Differentiation
- Well-differentiated: microvesicular foamy cytoplasm
- Moderately differentiated: some sebaceous differentiation
- Poorly differentiated: can be difficult to distinguish from other epithelial malignancies
- Oil red O or Sudan black stain intracytoplasmic lipid in fresh tissue (frozen section) and is diagnostic
- Morphology
- Lobular: basaloid features
- Comedoca: central necrotic foci
- Papillary: tumor cells in fronds with foci of sebaceous-differentiated cells
- Dissemination
- Pagetoid: individual or clusters of cells invade within the epidermis or conjunctival epithelium
- Direct extension: intralymphatic, may include perineural invasion
- Vascular invasion: a distant metastasis after a regional lymph node
- Sebaceous carcinoma in situ: conjunctival epithelium completely replaced by tumor cell
- Worse prognosis
- Upper lido>10mm in diameter
- Meibomian gland origin
- Symptoms > 6 months
- Infiltrative growth
- Moderate to poor differentiation
- Multicentric with pagetoid, lymphatic, or vascular invasion
Nick’s tips: A diffuse sebaceous carcinoma can mimic blepharoconjunctivitis, whereas a focal lesion can be confused with a recurrent chalazion clinically. Any loss of lashes should alert you to a more insidious process occurring.
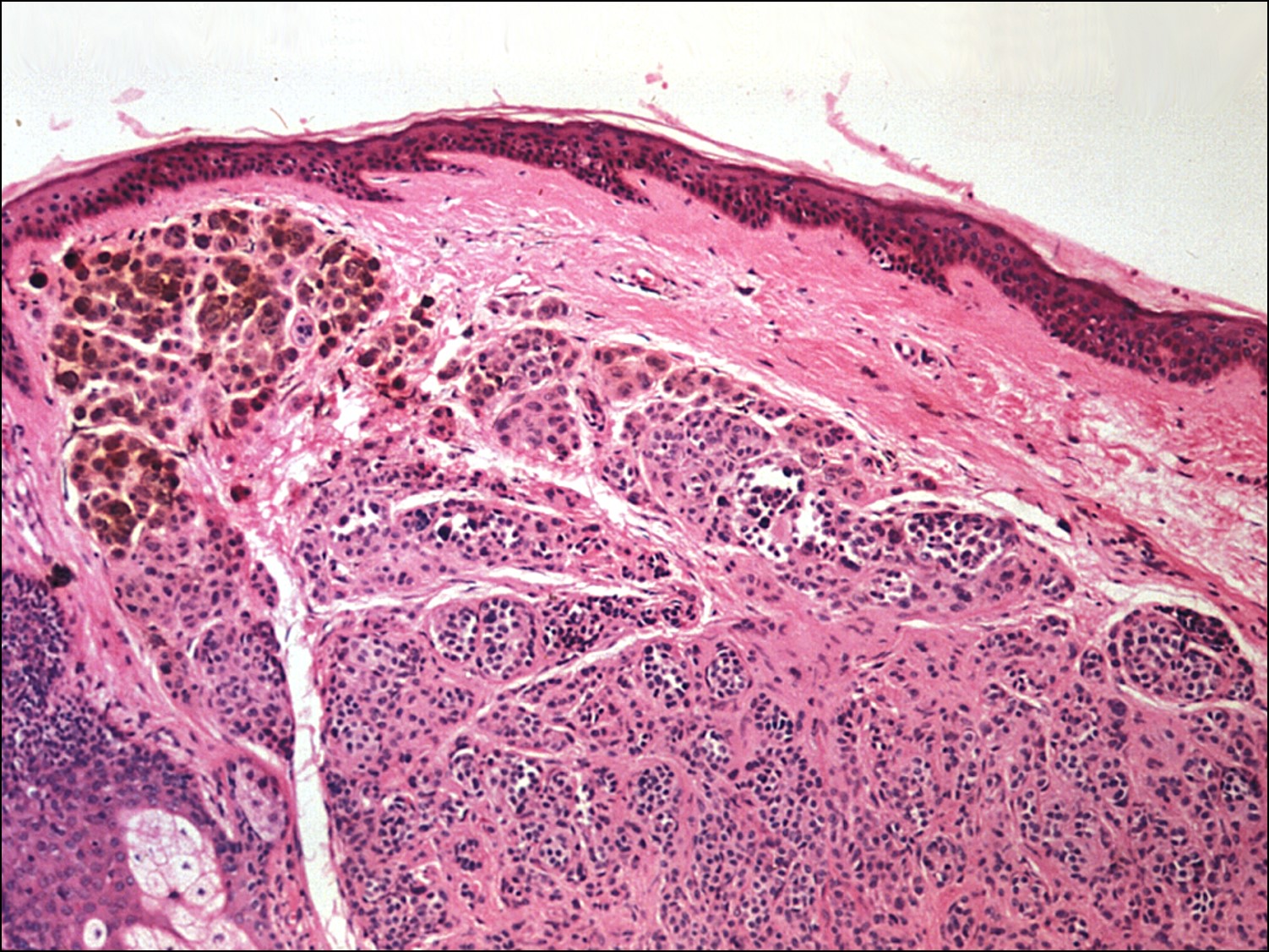
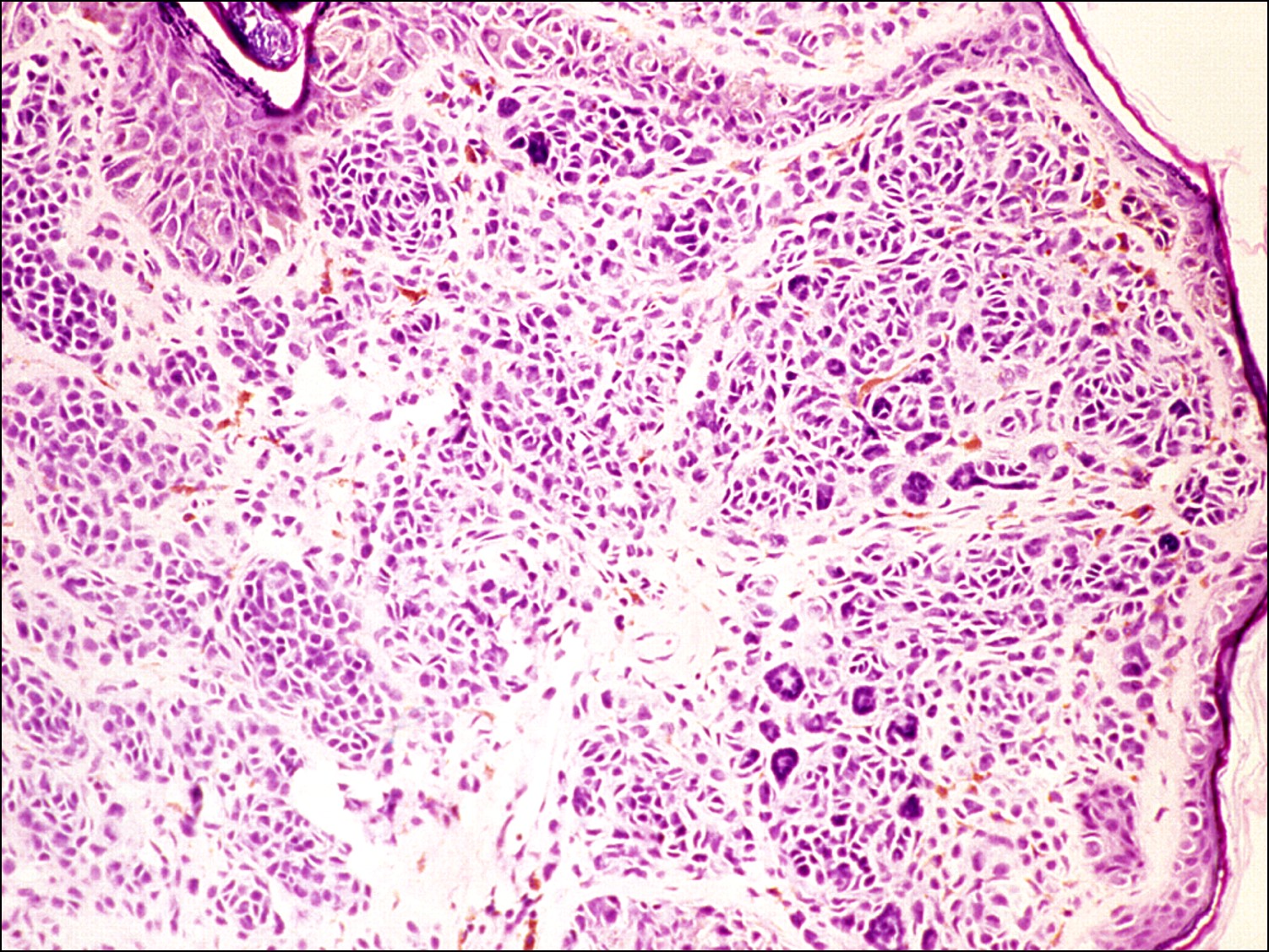
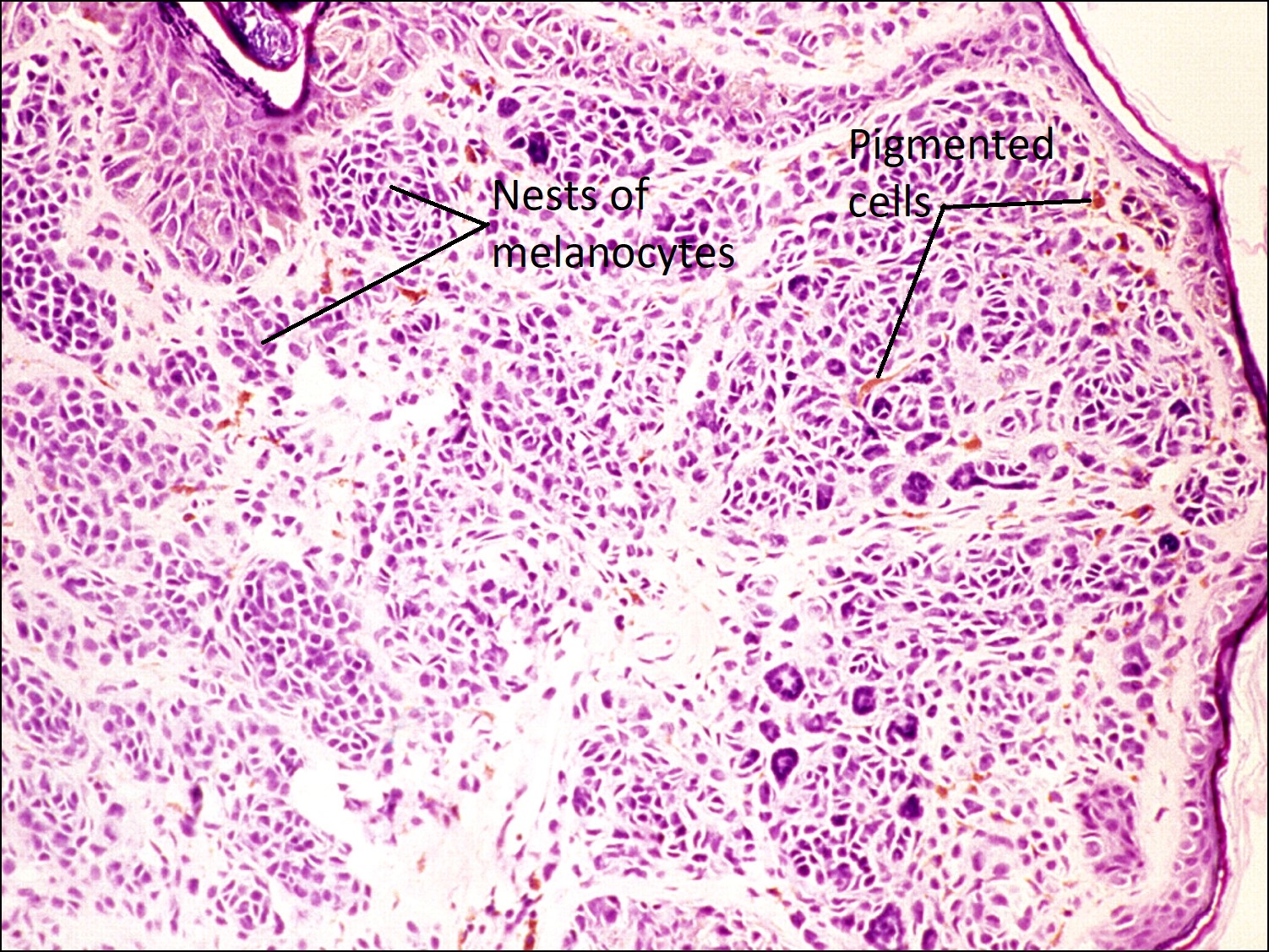
Nevus of the Eyelid (Junctional, Compound, Intradermal)


Nevus of the eyelid margin

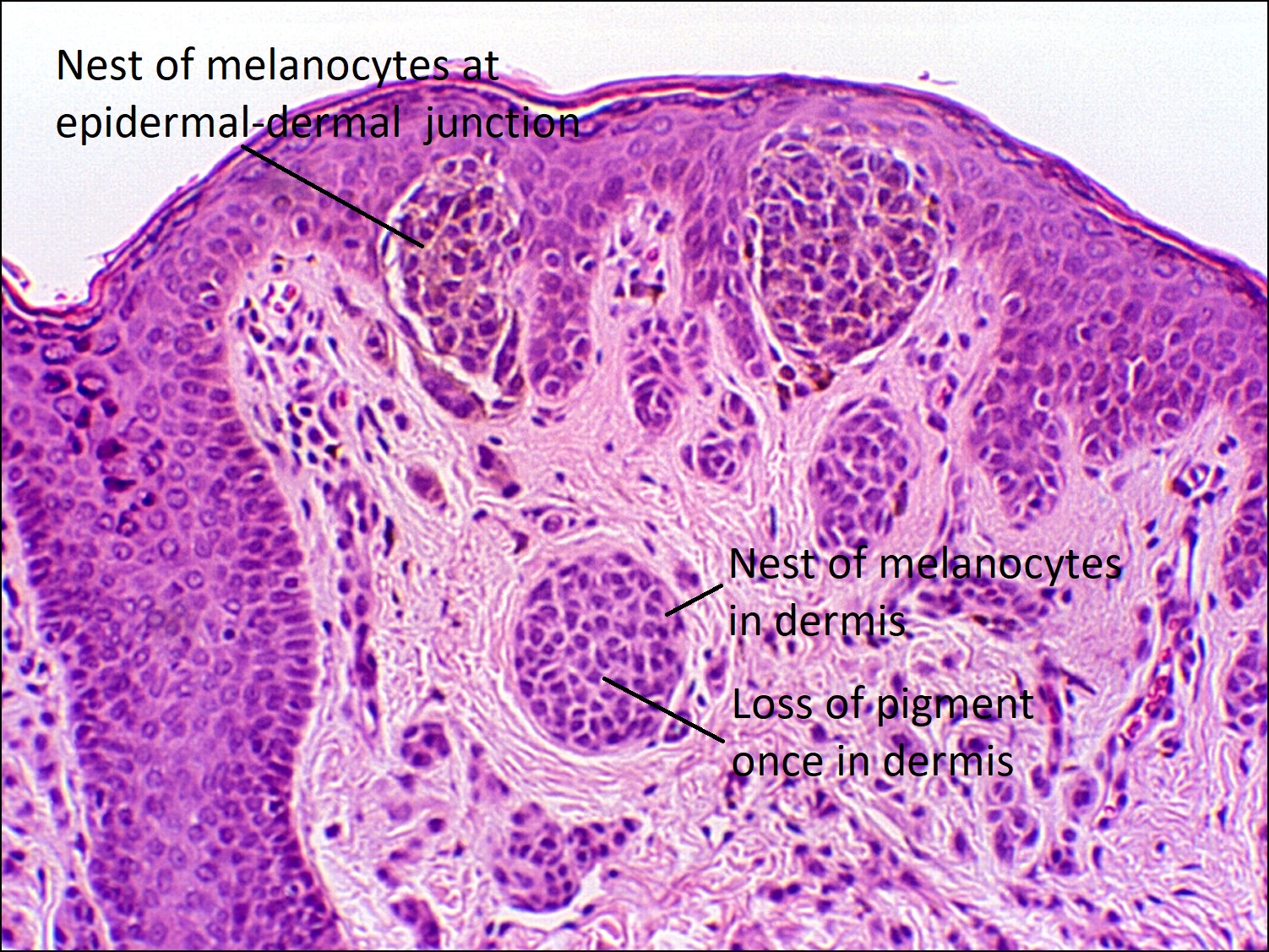
Compound nevus
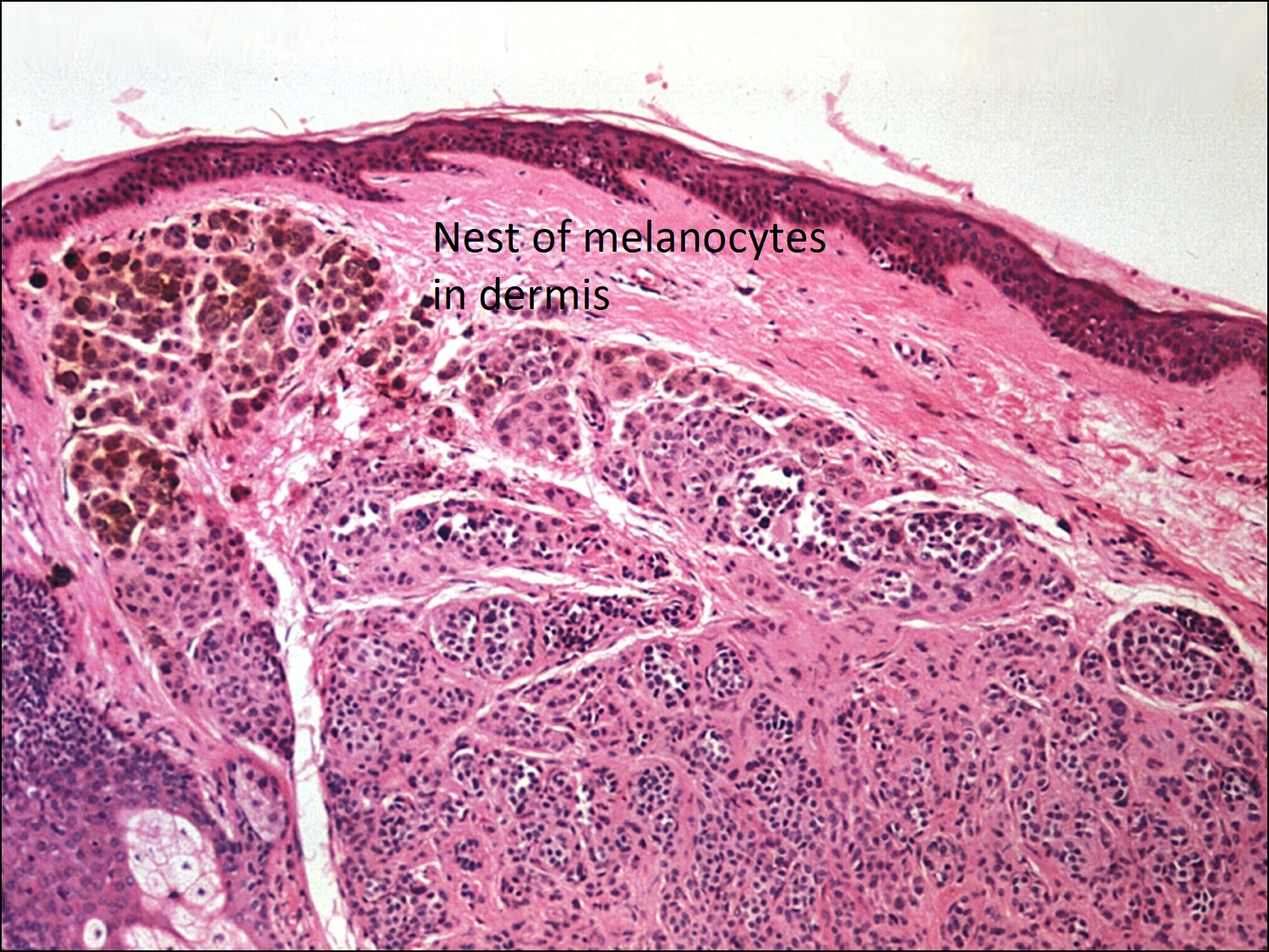
Dermal nevus
- Benign neoplasm of melanocytes
- Congenital nevi: present at birth
- Typically larger
- Giant congenital melanocytic nevi: nevi > 20cm in diameter
- Risk of melanoma proportional to size
- Require close follow-up and possible excision
- Kissing nevus: nevus develops during lid fusion (Week 18 to Month 5) and involves both upper and lower lids
- Nests of pigmented melanocytes classified by their location within the skin
- Junctional: nevus cells at epidermal-dermal junction
- Clinically appear flat, retains some malignant potential
- Compound: nevus cells at junction and in the superficial dermis
- Clinically appear raised and may increase in pigmentation
- Retains some malignant potential, but less than junctional
- In children, migrating melanocytes pull epithelium down with them, forming epithelial cysts
- Presence of a nearby epithelial cysts indicates nevus present at birth (congenital) or in early childhood
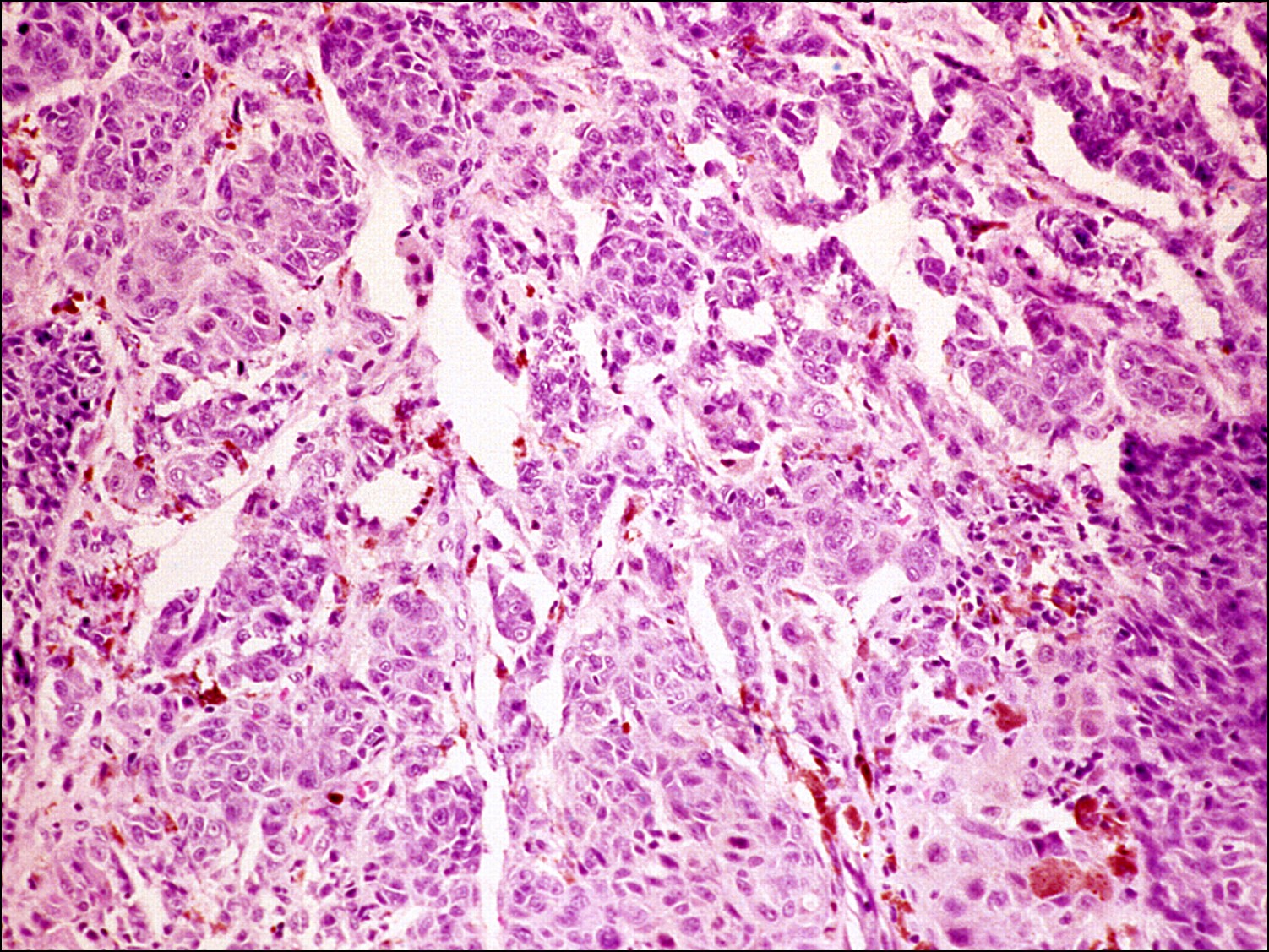
- Dermal: nevus cells only within the dermis
- Can become amelanotic
- Giant multinucleated nevus cells and adipose tissue indicate older nevi
- Malignant potential is lost
- Junctional: nevus cells at epidermal-dermal junction
- Intradermal nevus cell classification
- Type A: upper dermis, polygonal or epithelioid shape
- Type B: middle dermis, lymphocyte-like, smaller cell with less cytoplasm
- Type C: deep dermis, spindle-shaped, resemble Schwann cells, little to no melanin
- Variants
- Balloon cell nevi: large, foamy or finely vacuolated melanocytes without atypia
- Spindle/epithelioid nevi: compound nevus in children and young adults
- Blue nevi: pigment in dermal melanocytes
- Freckle: pigment in basal layer of epidermal melanocytes
- Atypical variants
- Spitz nevus
- Develop in late childhood or adolescence
- Larger, up to 1.0cm
- Tan-pink color
- Compound
- Pleomorphic
- Enlargement of nucleus and cytoplasm
- No atypical mitotic figures, no intraepidermal migration, no lack of maturation
- Increased risk of melanoma
- Treatment: complete excision
- Dysplastic nevus
- Size greater than 0.5cm
- Irregular margins, irregular pigmentation
- Atypia: nuclear enlargement, hyperchromasia(darker nucleic staining), prominent nucleoli
- Treatment: complete excision
- Multiple dysplastic nevi: increased risk of melanomaand possible genetic predisposition, so examine family members as well
- Spitz nevus
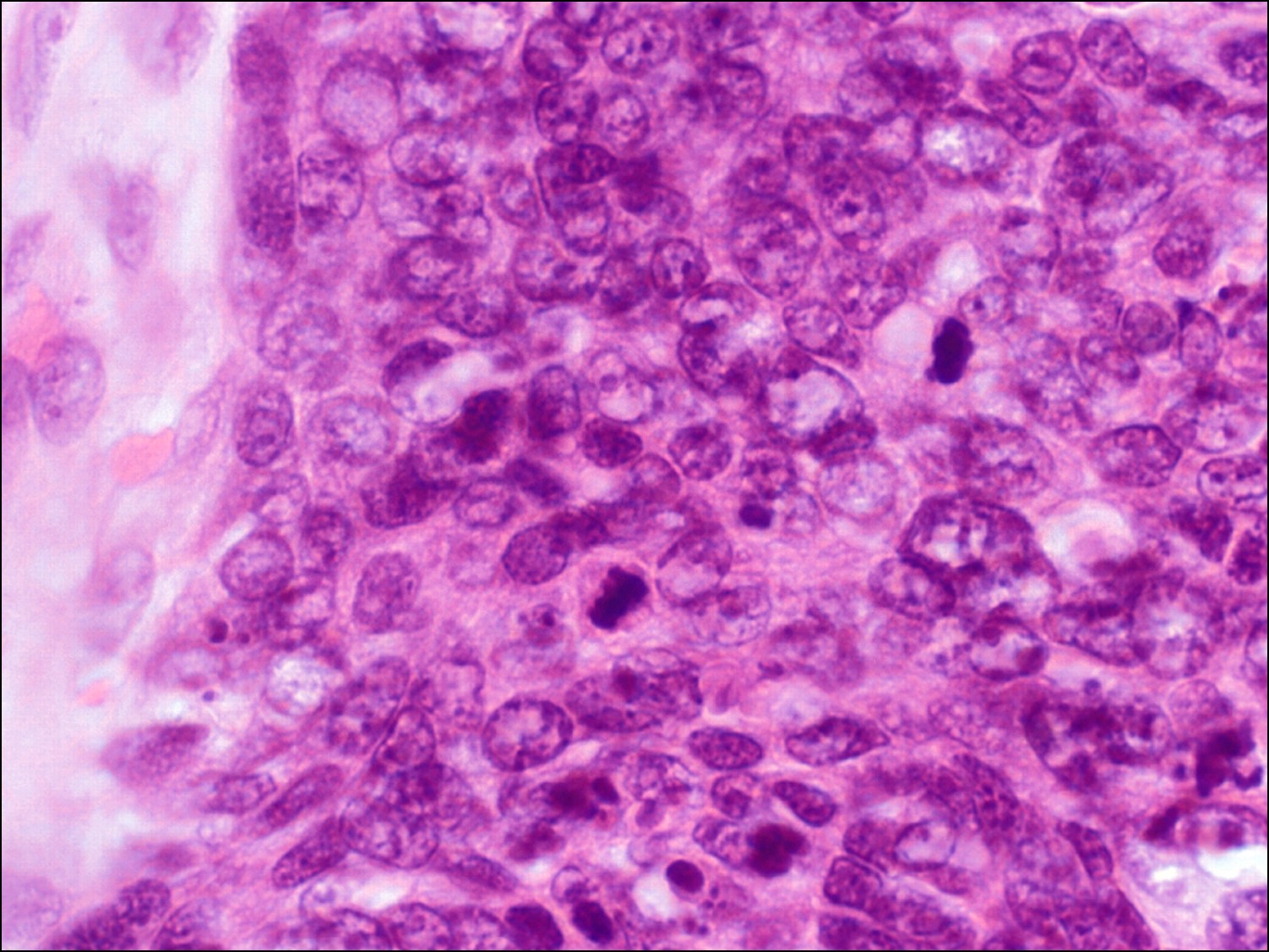
Melanoma of the Eyelid


Melanoma of the eyelid
Low magnification
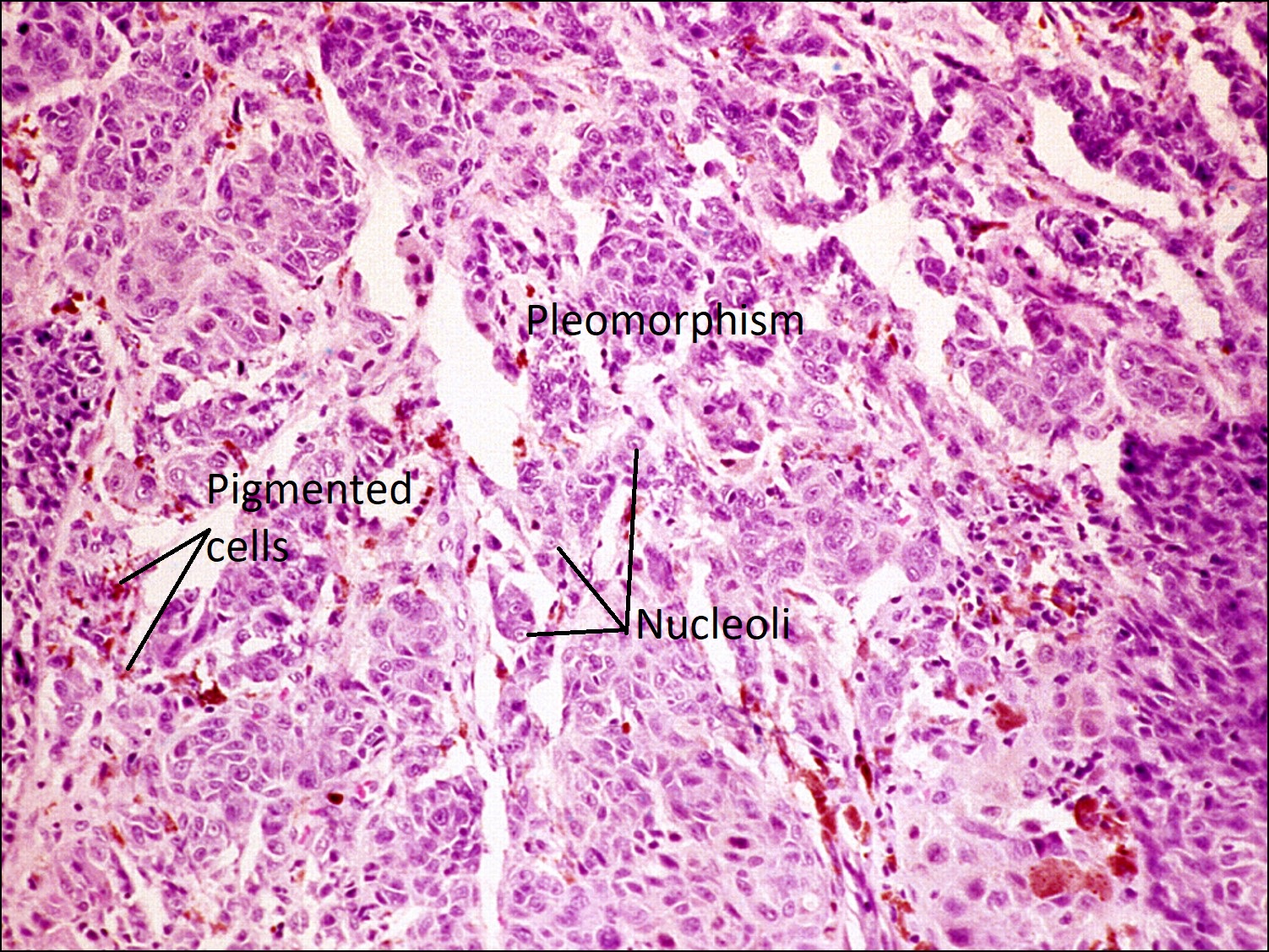
High magnification
- Rarely found in the eyelids, but lower lid more common than upper
- Can arise from pre-existing nevus or de novo
- Signs of malignancy
- Greater than 0.5cm in size
- Irregular margins, irregular pigmentation
- Change in color, size, or shape
- Atypical cells with nuclear enlargement, hyperchromasia, prominent nucleoli
- Vertical growth leading to an elevated or indurated mass
- Crusting, bleeding, ulceration, pain, itching, tenderness
- Types
- Lentigo maligna
- Most common type on the eyelids
- Occurs on the sun-exposed skin of the face in the elderly
- Develops from preinvasive lesion (Hutchinson’s melanotic freckle)
- Flat macule with variable pigmentation
- Hyperplastic radial growth along the basal epidermis of atypical pleomorphic melanocytes
- Follow along outer sheaths of hair shafts
- Superficial spreading
- Most common type of cutaneous melanoma
- Occurs on unexposed skin, typically upper back and legs, of individuals in their 50s
- 50% arise from nevi
- Pigmented macule with irregular outline and palpable borders
- May have white regions signifying spontaneous regression
- Pagetoid spreading of tumor cells in radial growth pattern close to the epidermal-dermal junction
- Nodular
- Occurs in middle-aged patients with men twice as common as women
- 20% arise from nevi
- Rapidly growing blue-black or amelanotic pedunculated nodule
- Narrow intraepidermal component
- Prominent intradermal vertical growth, therefore more deeply invasive
- Acral-lentiginous
- Involves extremities (palms and soles) and not eyelids
- Similar to lentigo maligna melanoma, but atypical cells also in superficial epidermis
- Radial growth
- Lentigo maligna
- Lymphocytic response at base of lesion more likely to be seen in melanoma rather than a nevus.
- Prognosis
- Change in lid margin, madarosis, or conjunctival involvement means worse prognosis
- In Stage I (localized) disease, prognosis correlates with depth of invasion
- Breslow depth: measurement from upper layer of epidermis to deepest margin of the tumor in millimeters
- Can metastasize to lymph nodes
- Treatment
- If no metastatic disease, wide excision with regional lymph node removal
- Stage II: can consider sentinel lymph node biopsy
- Stage III and IV: additional chemotherapy and radiation therapy
Lymphoma

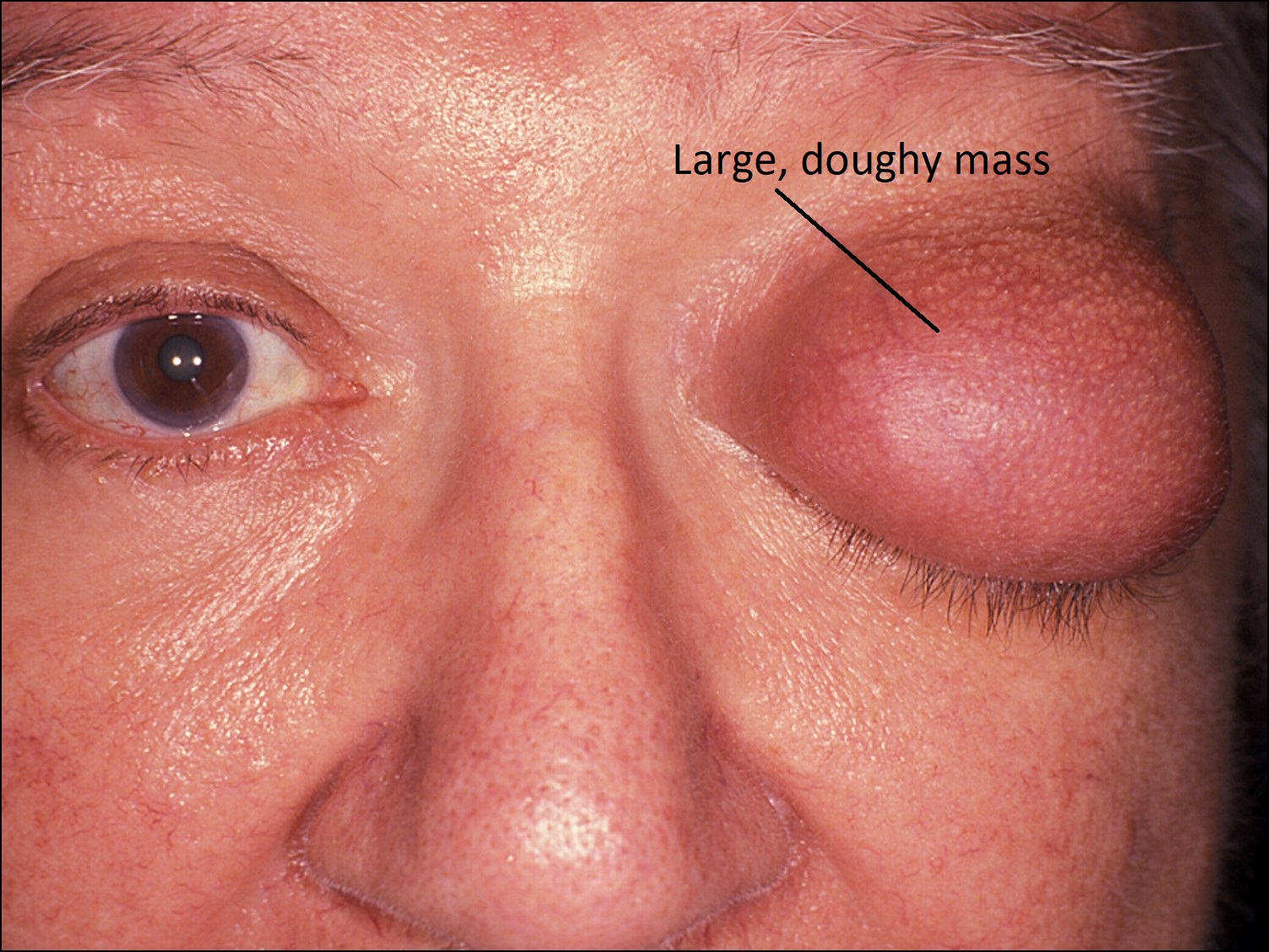
External photo
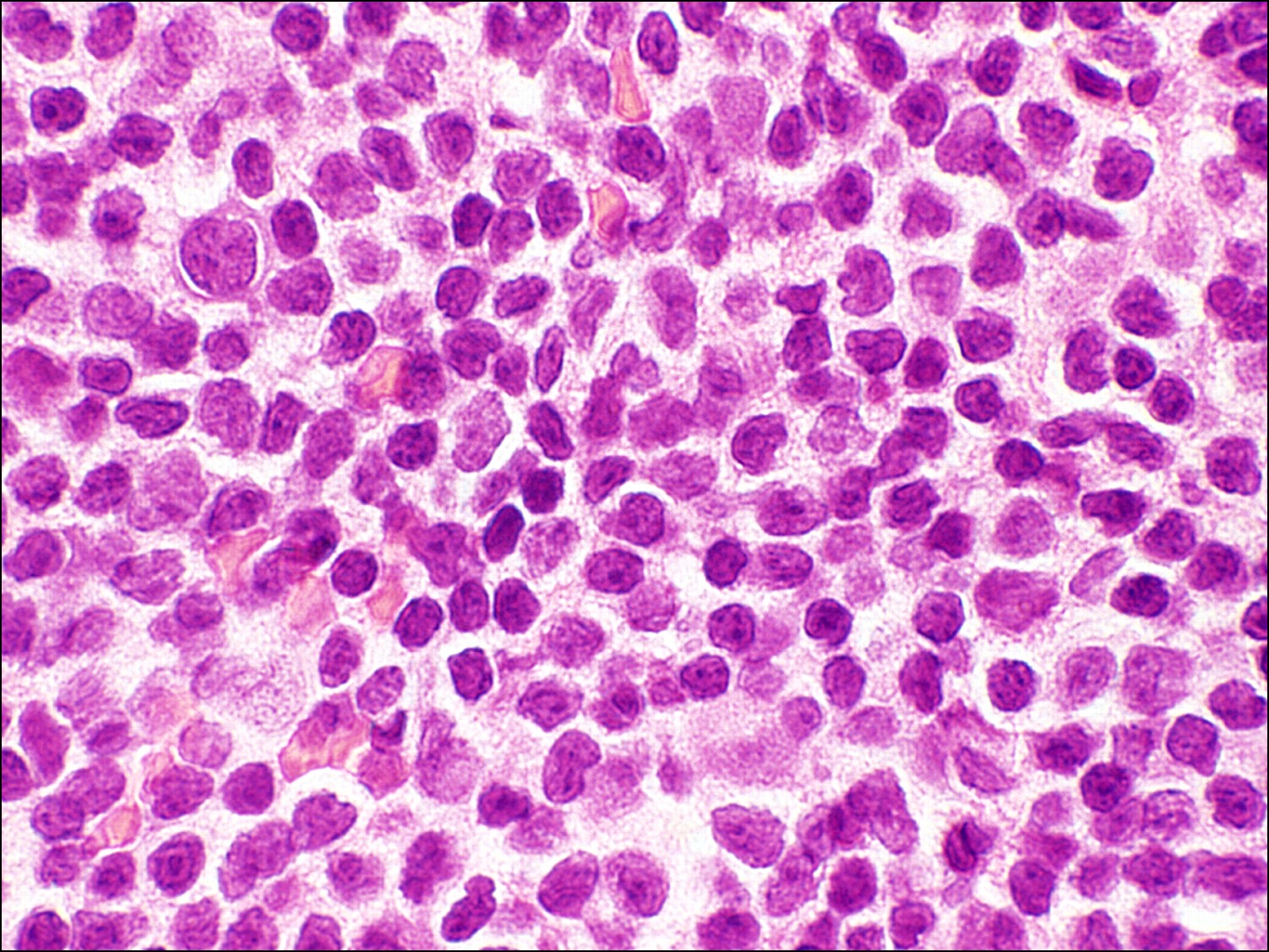
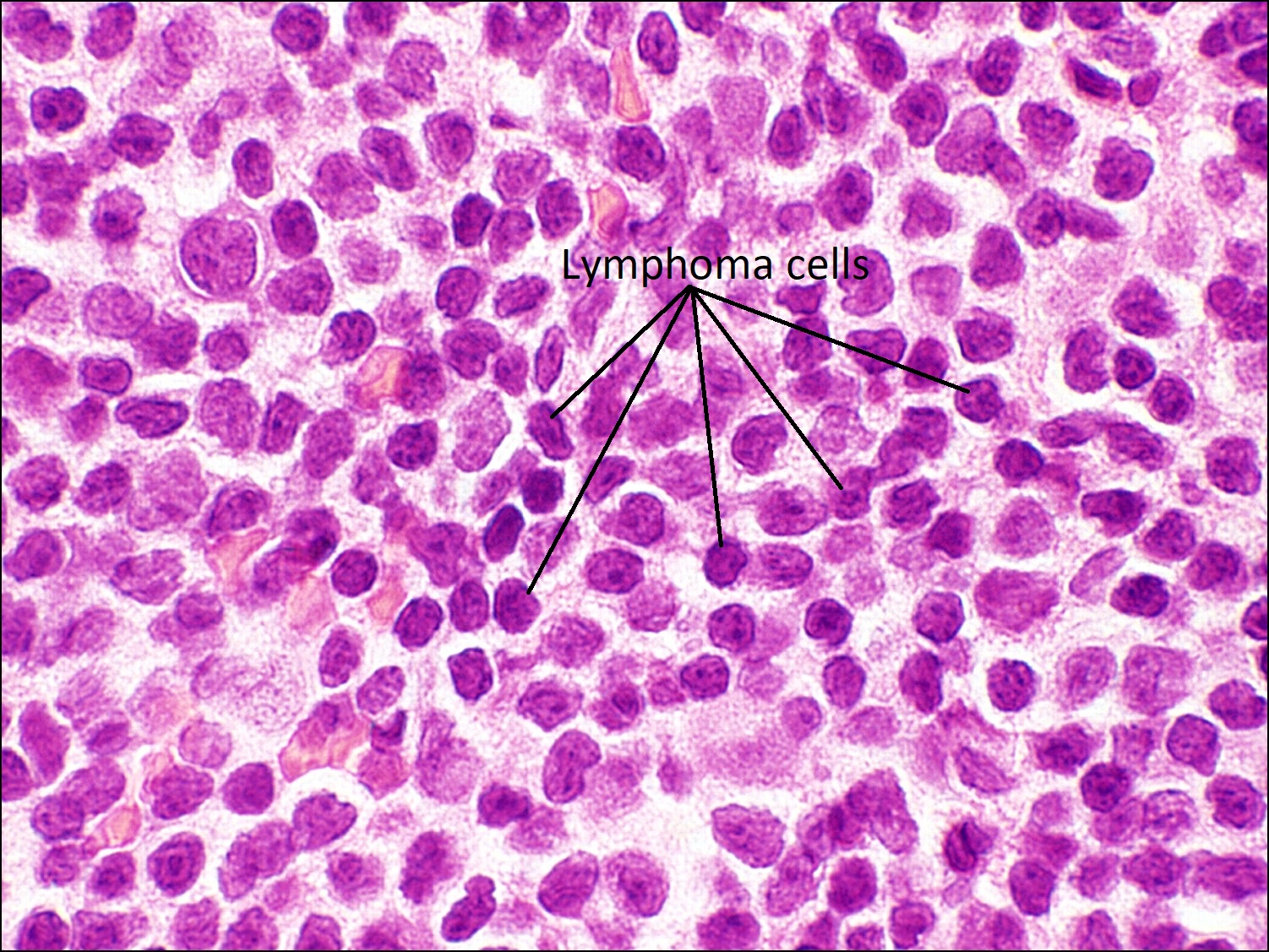
Lymphoma of the Eyelid
- Doughy mass of the eyelid
- Does not feel hot or as if an acute infectious process is taking place
- When in the eyelid, it is usually secondary to continuous spread from an orbital lymphoma
- Most orbital lymphomas are Mantle Cell lymphomas of B-cell origin
- Rare tumor of the eyelid
- Abundant lymphocytes (basophilic nuclei with scant cytoplasm) on histology
- Lymphoma cells are not organized into follicles
- Stains positive for CD20, CD5, and Cyclin D1
- Monoclonality of cells can be confirmed with immunohistochemistry
Merkel Cell Carcinoma


External photo
Merkel Cell Carcinoma
- Fleshy, reddish-blue lesion
- Very rare tumor of the eyelid
- Most commonly arise on sun-exposed areas of the head, neck, trunk, arms, and legs
- Round cells look like large cell malignant lymphoma cells
- High number of mitotic figures
- On electron microscopy, can see dense cytoplasmic neurosecretory granules
- High rate of recurrence after excision
Mucinous Adenocarcinoma


Mucinous adenocarcinoma


Mucicarmine stain
- Rare tumor of the eyelid
- Islands of tumor cells swimming in sea of mucin
- Mucicarmine stains mucin pink or red and nuclei green
- If primary lesion, can treat with wide local excision
Capillary Hemangioma


Late Capillary hemangioma


High magnification
- Most common benign orbital tumor in children
- May present at birth or within the first 6 months of life and grow slowly over time
- Form of hamartoma, a benign growth of normal tissue in a normal location
- More often present in the upper lid
- Early lesions: very cellular, solid nests of endothelium, few vascular lumens
- Late lesions: lobular arrangement of well-developed, flat, endothelium-lined vascular channels
- Involuting lesions: increased fibrosis and hyalinization of vascular walls with lumen occlusion
- Spontaneously resolve by school age
Syringoma


Syringoma
- Benign tumor of eccrine ducts commonly seen in young women
- Multiple tiny, waxy, yellow papules on the lower eyelid
- Characteristic tadpole-or comma-shaped bilayered epithelium with central lumen containing colloidal material resemble paisley pattern
- Dense sclerotic stroma
References:
Harper RA. Basic Ophthalmology. Amer Academy of Ophthalmology; 2010.
Yanoff M, Fine BS. Ocular Pathology, A Text and Atlas. Lippincott Williams & Wilkins; 1989.