


Hyphema
Home / Basic Ophthalmology Review / Trauma
Title: Hyphema
Author: Bryan Thiel, MS4 – University of Central Florida College of Medicine
Images
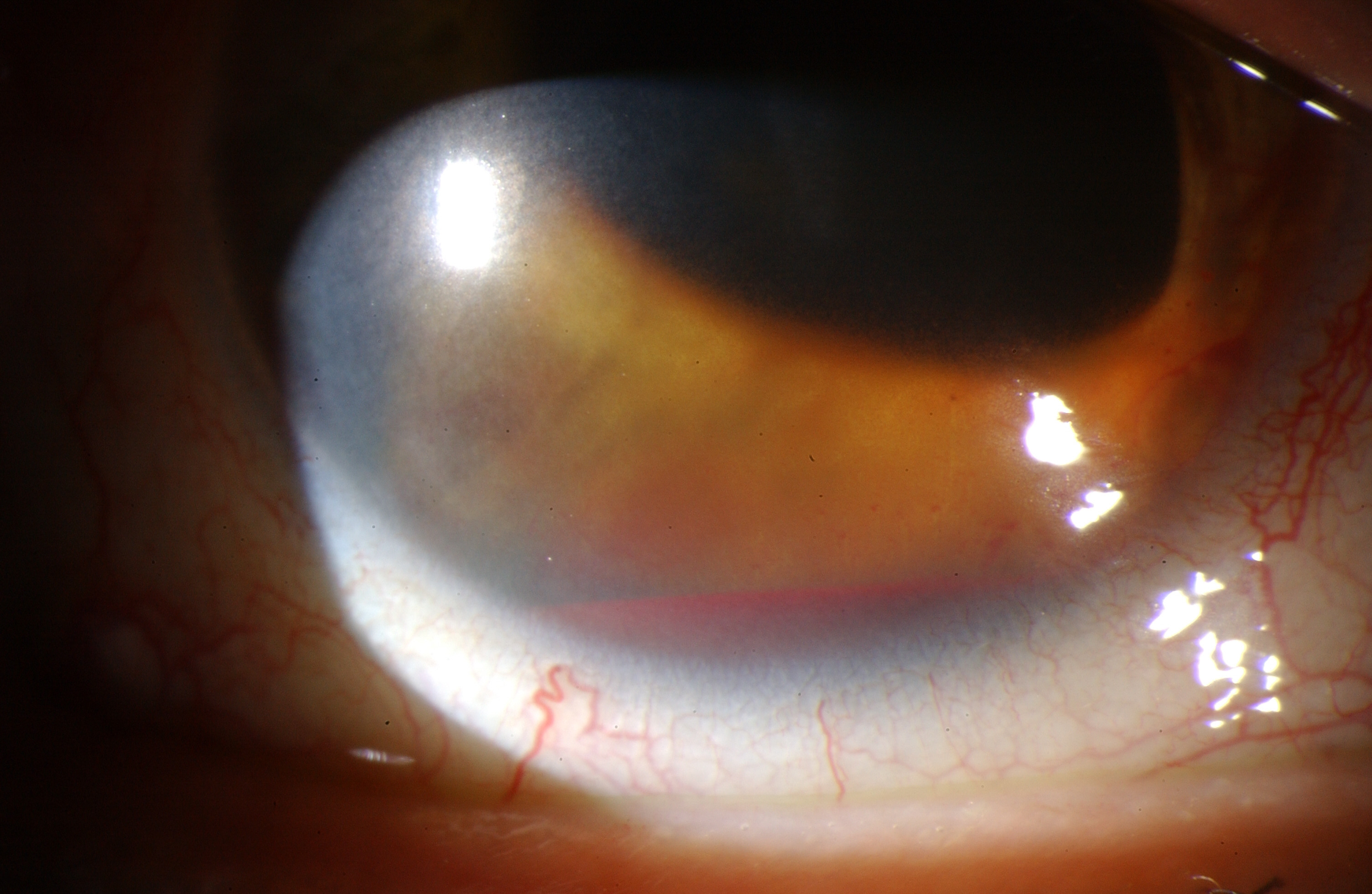
Grade I Hyphema with cells visible floating in the anterior chamber

Grade III hyphema or 60% fill hyphema with ciliary flush or conjunctival injection

Post-surgical hyphema after a cataract extraction and intra-ocular lens placement.
Introduction
Hyphema refers to the presence of red blood cells in the anterior chamber of the eye. This is not to be confused with hypopyon which refers to the presence of white blood cells in the same compartment. Hyphemas most commonly arise secondarily to blunt trauma to the globe due to shearing of the small vessels supplying the iris, ciliary body and trabecular meshwork. The severity of the hyphema can either be measured by the depth of settled red blood cells at the base of the anterior chamber or graded on a scale of zero to four as below (Table 1).
Table 1. Grading System of Hyphemas
| Grade 0 or “microhyphema” | Rare cells visible only in slit lamp examination, no layering of cells |
| Grade I | Layering of cells at base of anterior chamber, measuring less than ⅓ the total space |
| Grade II | Layering of cells at the base of the anterior chamber, measuring between ⅓ and ½ the total space |
| Grade III | Layering of cells at the base of the anterior chamber, measuring greater than ½ the total space but not occupying its entirety |
| Grade IV | Layering of cells that occupy the entire total space of the anterior chamber, also called “8-ball” or “black ball” hyphema |
Presentation
Patients will not typically present with complaints of “seeing red” or having “blood in the eye” but rather will have had recent trauma to the globe with symptoms including pain, photophobia and blurred vision. It is imperative to confirm the mechanism of injury, medication use (i.e. anti-platelets, anti-thrombotics) and family history of sickle cell disease or coagulopathy, as these may contribute to the severity of the bleed. A comprehensive eye exam is mandatory in every case of hyphema looking for other sequela of trauma such as ruptured globe, traumatic optic neuropathy or retinal detachments.
Differential
While trauma is the most common source of hyphemas, it is important to keep a broad differential as this symptom may be an early indicator for the following conditions:
Post-surgical hyphema: Surgical manipulation of the anterior structures of the eye may result in bleeding.
- Diabetes: blood in the front of the eye could be a result of ruptured friable vessels that grow on the iris and in the angle in response to long-term retinal ischemia from diabetic retinopathy.
- Intraocular tumors: including, but not limited to, retinoblastomas, iris and ciliary body melanomas and intraocular metastatic malignancies.
- Less commonly: herpetic keratouveitis, rubeosis iridis, juvenile xanthogranuloma, leukemia.
Management
Currently, there is no designated protocol for medical management of hyphemas. Medicinal eye drops such as corticosteroids (e.g. prednisolone acetate) and cycloplegics (cyclopentolate or atropine) are most commonly used. Fibrinolytics, such as aminocaproic acid (ACA) and tranexamic acid (TA), have been extensively discussed in the literature, however sensitivity analyses have demonstrated that these medications minimally reduce the risk of secondary bleeding. Therefore, these drugs have fallen out of favor for treating hyphemas. Patients with hyphemas may develop sudden jumps in their intraocular pressure (IOP) putting them at risk for glaucomatous optic nerve damage and significant discomfort. Therefore, IOP needs to be monitored daily for several days following the injury.
For cases of elevated IOP, first-line therapy includes the use of pressure-reducing medications. Of note, carbonic anhydrase inhibitors like dorzolamide are contraindicated in patients with sickle cell disease or trait, due to their effect on lowering pH which can induce sickling. All patients should be questioned about their sickle cell status and if there is any possibility the patient could have sickle cell disease, hemoglobin analysis testing should be ordered to ascertain disease status of the patient.
Due to the inherent association of hyphema with trauma, inflammation is classically seen in addition to red blood cells. Thus, topical steroids, in addition to cycloplegics, are commonly prescribed to reduce inflammation and the risk of development of iris synechiae (iris scarring to lens or cornea). It is important to keep in mind that once symptoms of inflammation have resolved, topical steroids should be tapered to reduce the risk of steroid-induced glaucoma.
In addition to medication, preventative measures such as placing strict activity restrictions, maintaining an elevated position of the head and using an eye shield are highly recommended to encourage settling of red blood cells and to reduce risk of secondary bleeds. Patients with non-resolving clots, corneal blood staining, or uncontrolled elevated IOPs may benefit from surgical evacuation of the clot or blood from the anterior chamber. All hyphema patients are at lifelong risk of glaucoma due to the damage to the trabecular meshwork from the injury and/or blood and need regular IOP checks for life.
References
- Gharaibeh A, Savage HI, Scherer RW, Goldberg MF, Lindsley K. Medical interventions for traumatic hyphema. The Cochrane database of systematic reviews.2013(12):Cd005431.
- Walton W, Von Hagen S, Grigorian R, Zarbin M. Management of Traumatic Hyphema. Survey of Ophthalmology. 2002;47(4):297-334.
Identifier: Moran_CORE_24622