


Optic Nerve
Home / Ophthalmic Pathology / Optic Nerve
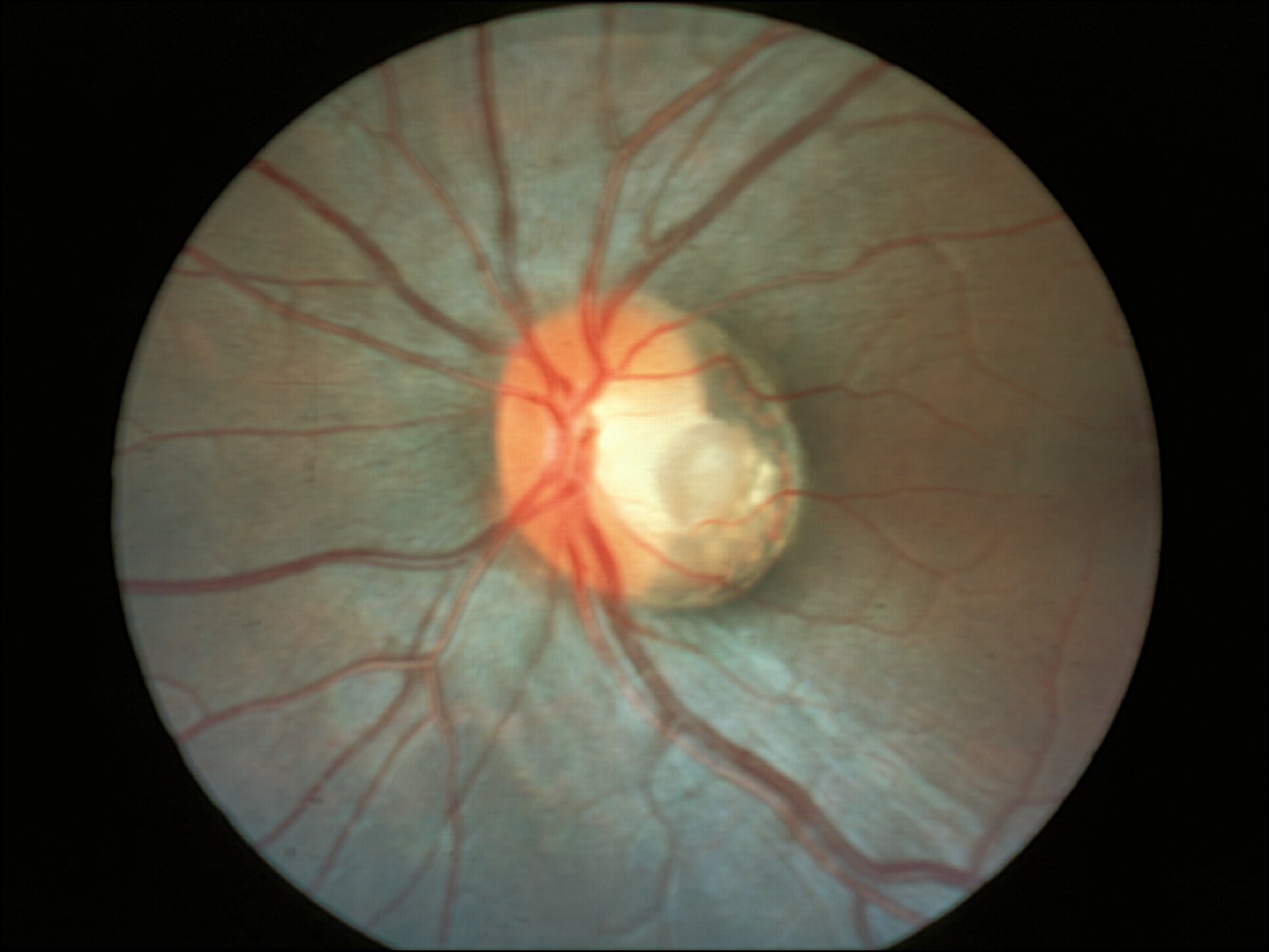
Normal Optic Nerve
Nick’s tips: The optic nerve is like a fiber-optic cable that carries visual information to the brain. The axons from the ganglion cell layer of the retina exit the eye through the lamina cribrosa, a fenestrate mesh-like area of the sclera. Once these axons pass through the lamina cribrosa, they become myelinated and take on the fiber-optic-like appearance. Each individual axon is myelinated by oligodendrocytes just as an individual optical fiber is coated in plastic. The fascicles of axons wrapped in pial septae is analogous to the bundles of optical fibers wrapped in further protective casing. Finally, the entire structure is encased in a protective sheathmade of dura mater for the optic nerve and steel for a fiber-optic cable.
The layers of the optic nerve from outer to inner are as follows:
- Dura mater = optic nerve sheath, continuous with the posterior sclera
- Arachnoid mater = comprised of meningothelial cells, source of meningiomas, carry blood supply to the nerve
- Subarachnoid space = contains CSF
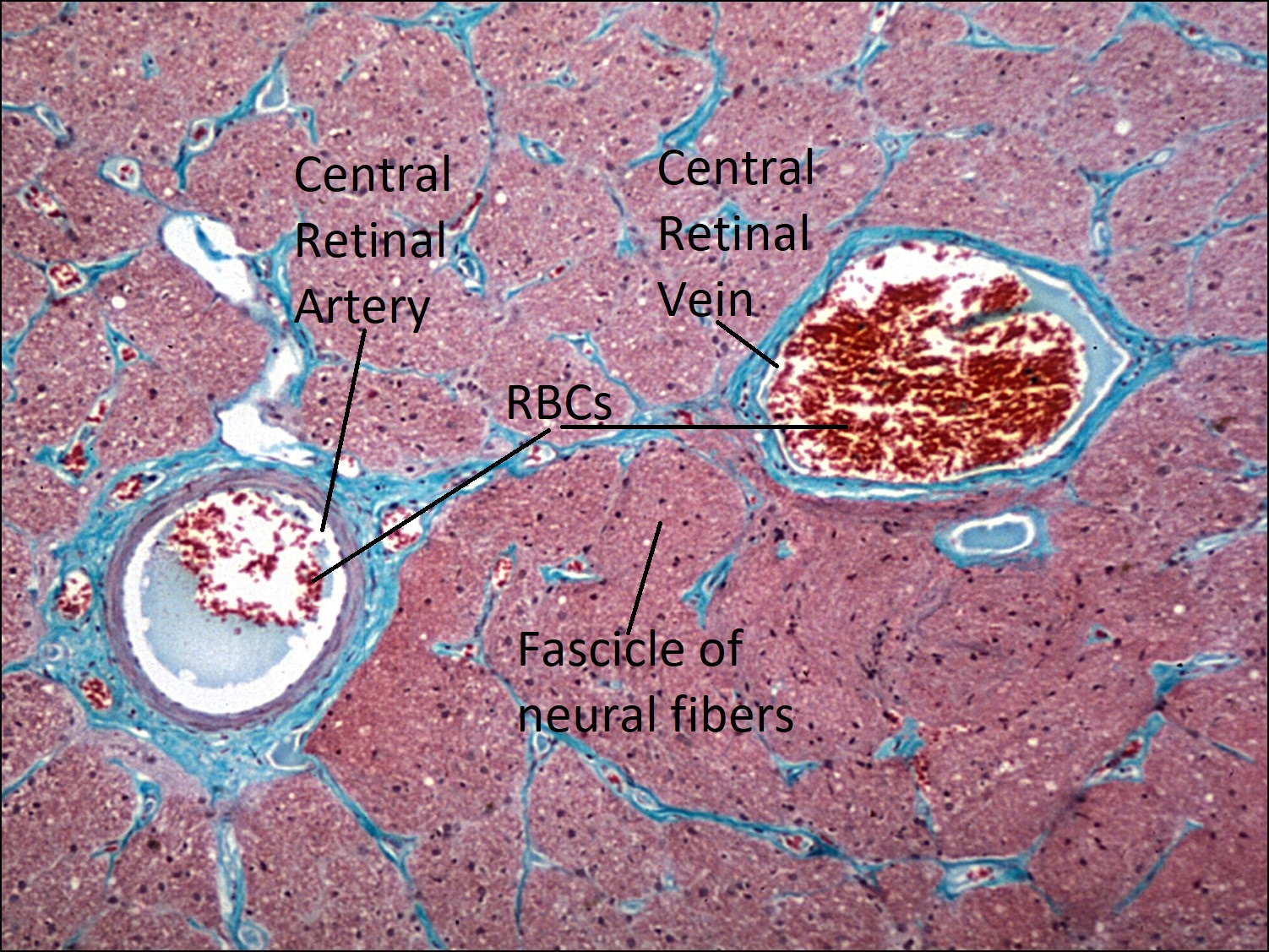
- Pia mater = forms connective tissue septae between bundles or fascicles of nerve fibers
- Nerve fibers = axons have their nuclei in the ganglion cell layer of the retina
- Support cells
- Astrocytes: provide nutrition, source of gliomas
- Oligodendrocytes: produce myelin
- Microglial cells: phagocytic cells of the CNS
- Support cells
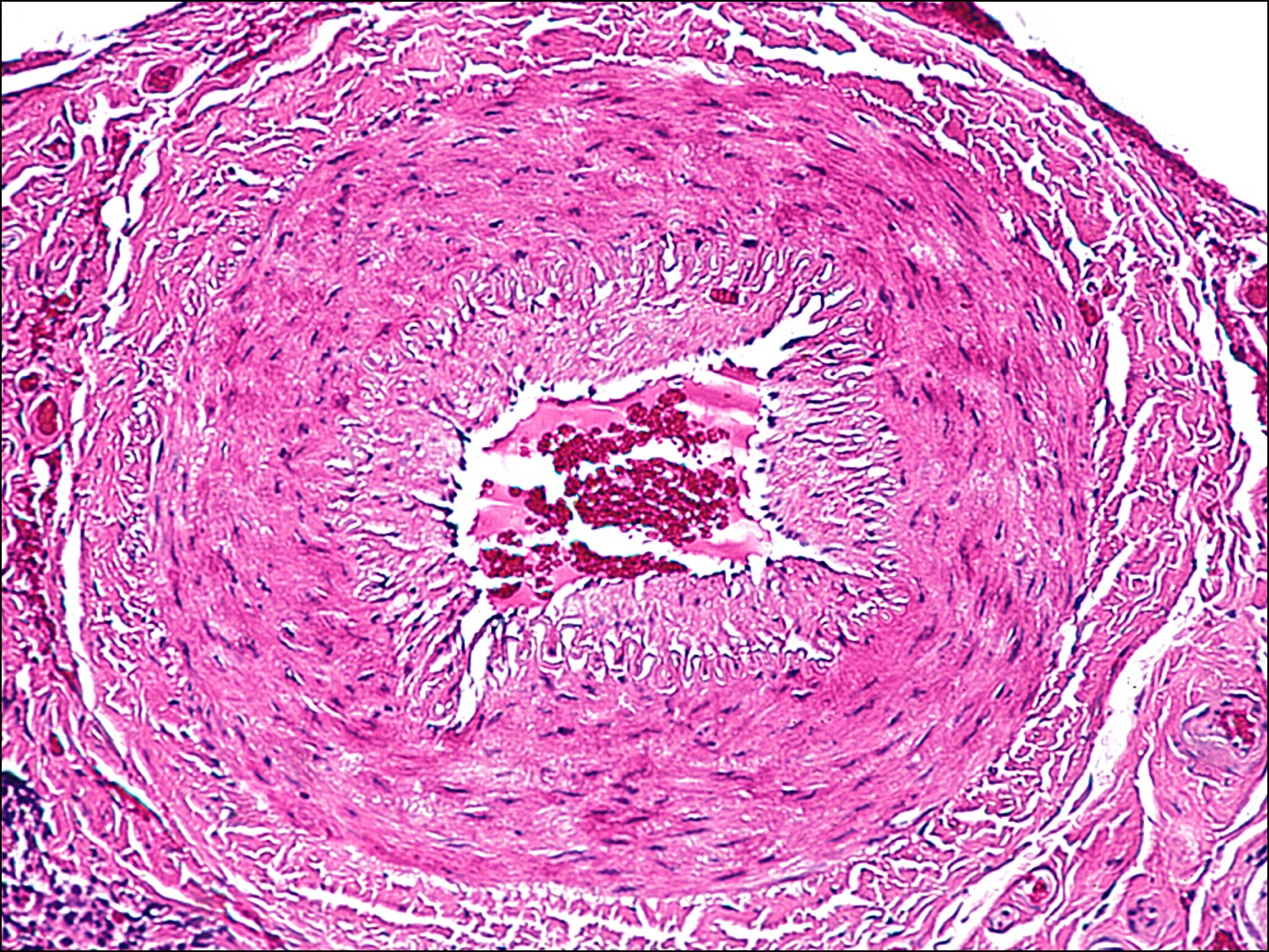
- Central retinal artery and vein: The distance between these vessels decreases as you approach the lamina cribrosa.
- The central retinal artery is typically nasal to the vein
- They share a common adventitial sheath

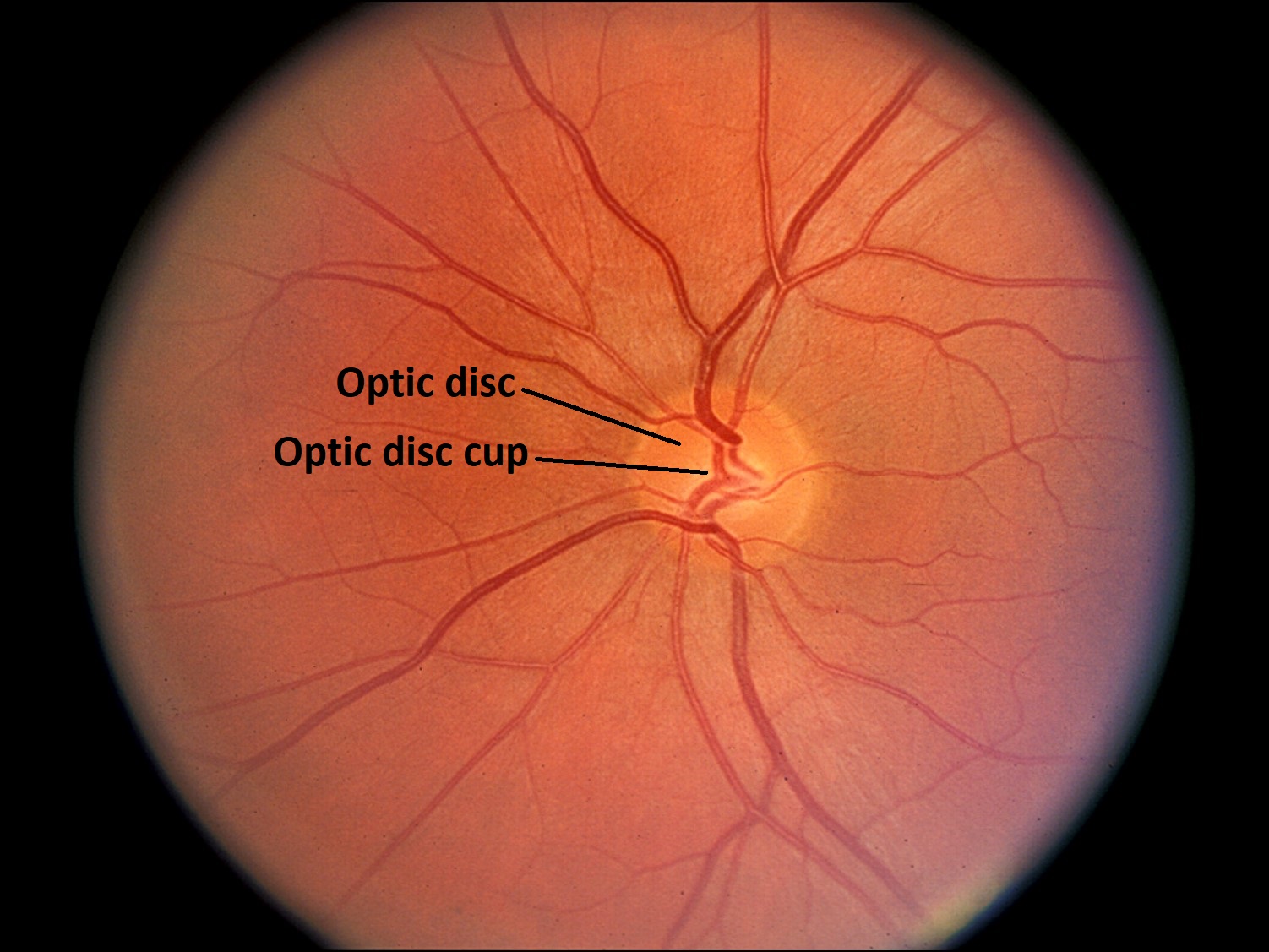
Fundus photo of normal optic nerve
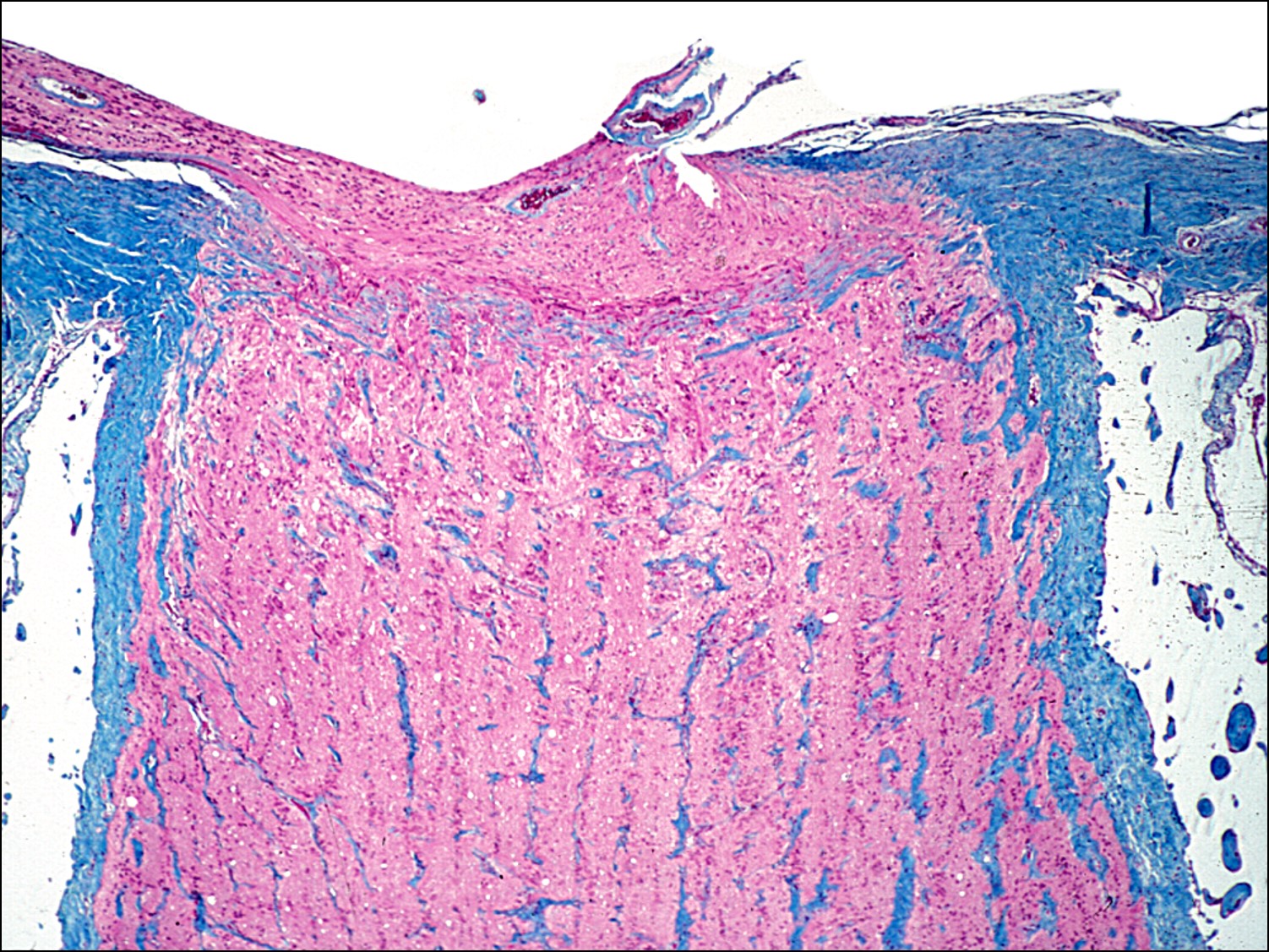

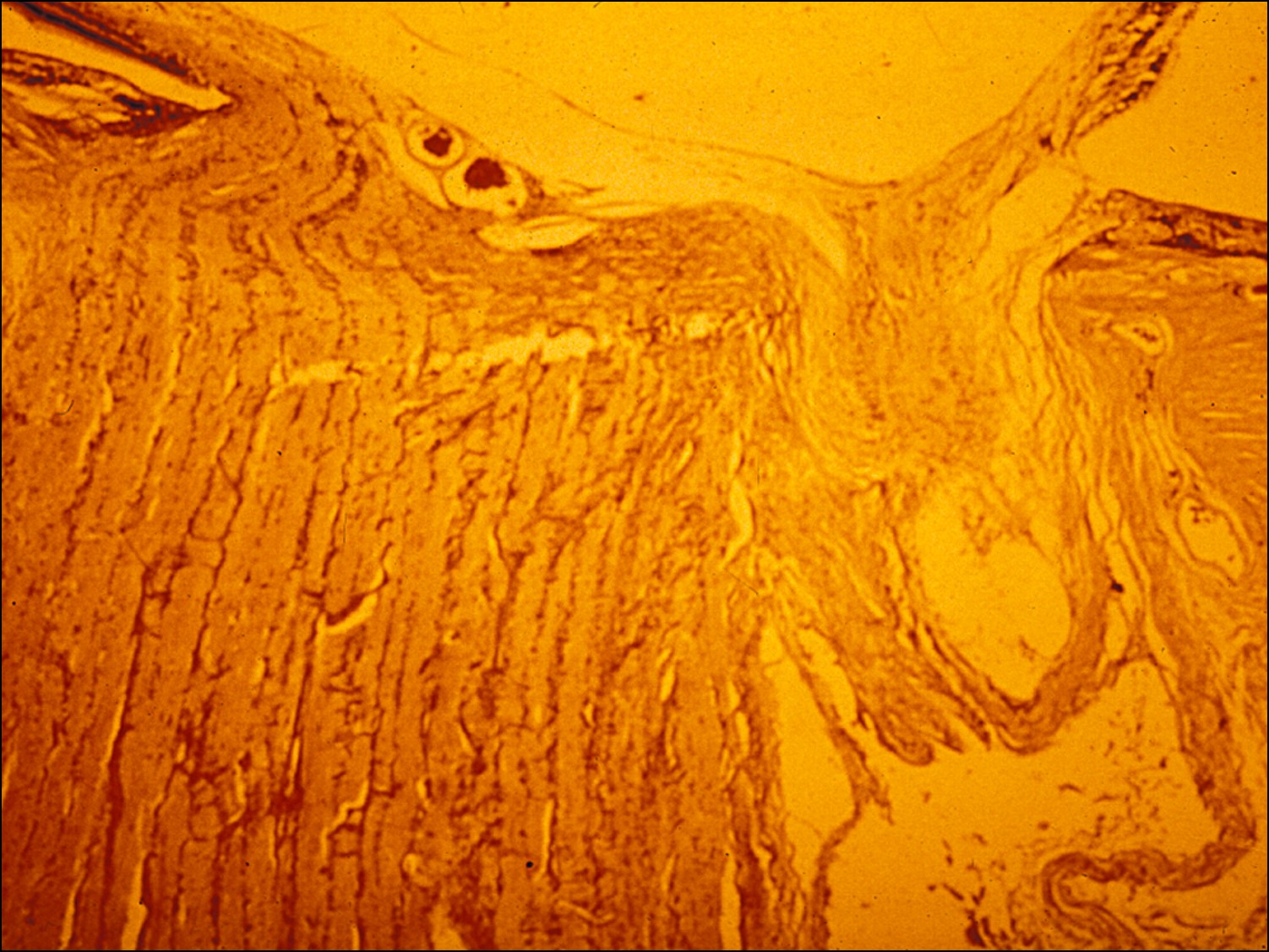
Trichrome stain optic nerve

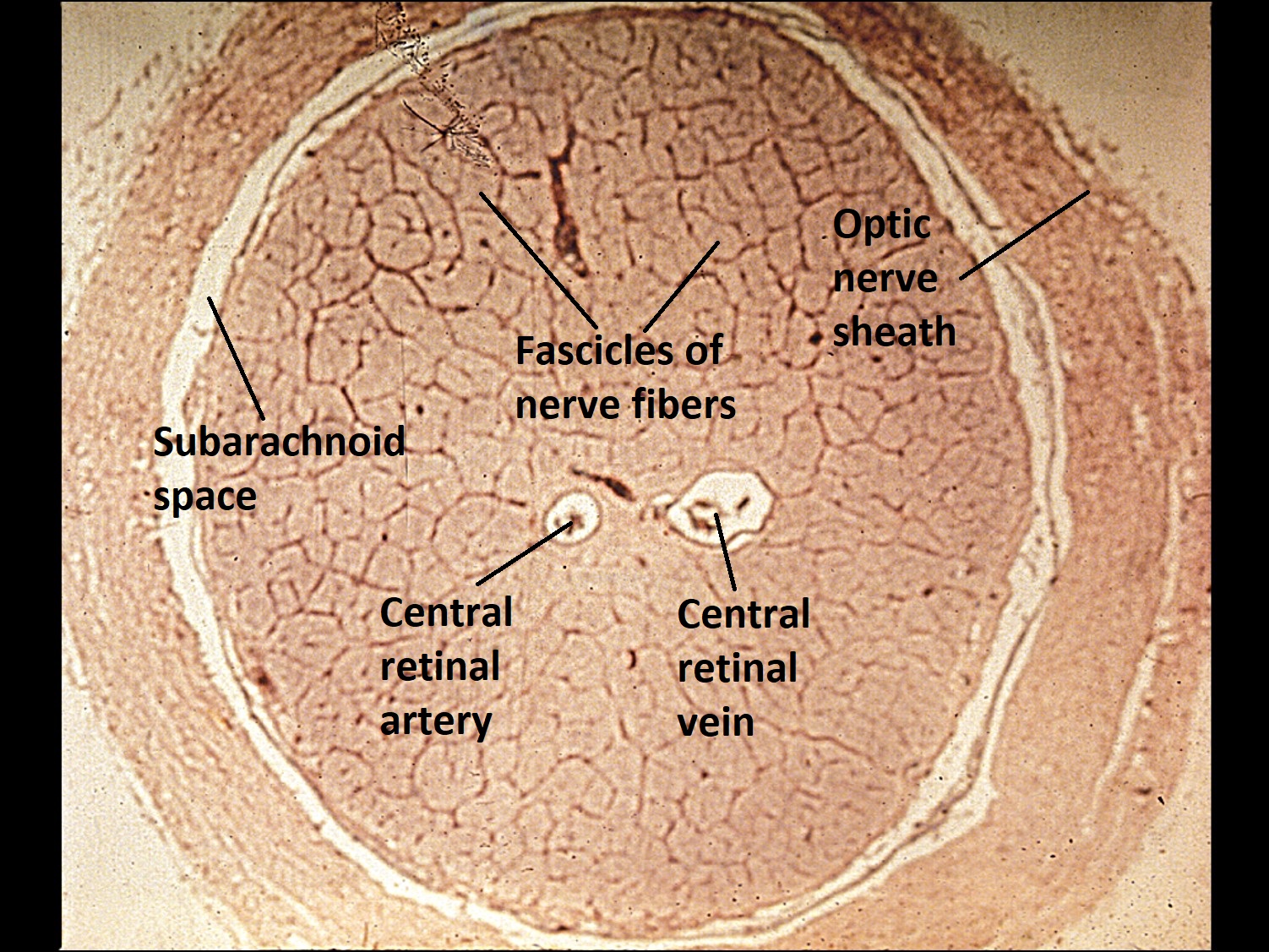
Cross-section of optic nerve


Optic Nerve Sheath


Support cells of the optic nerve
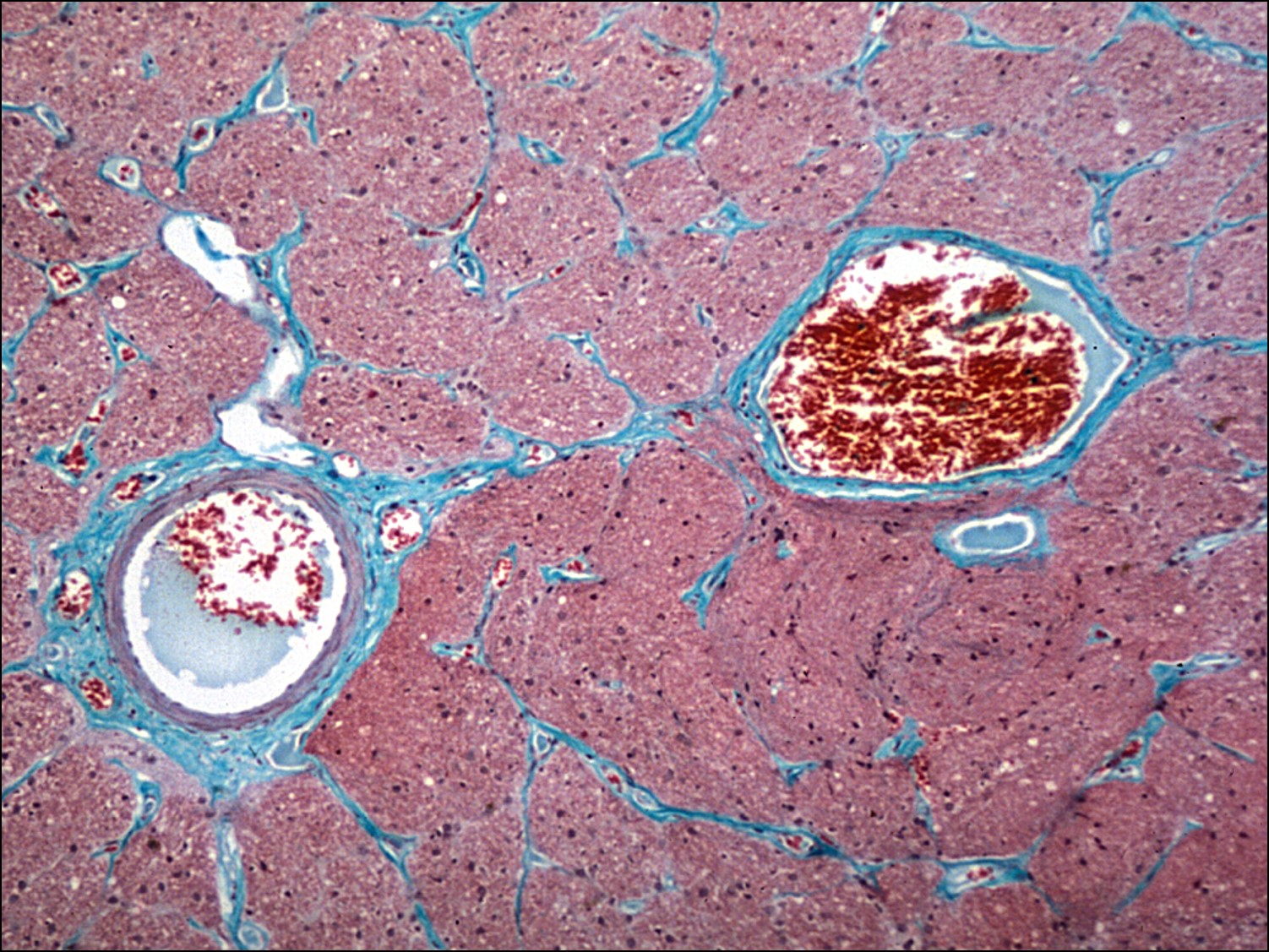
Central Retinal Artery & Vein
Optic Nerve Coloboma

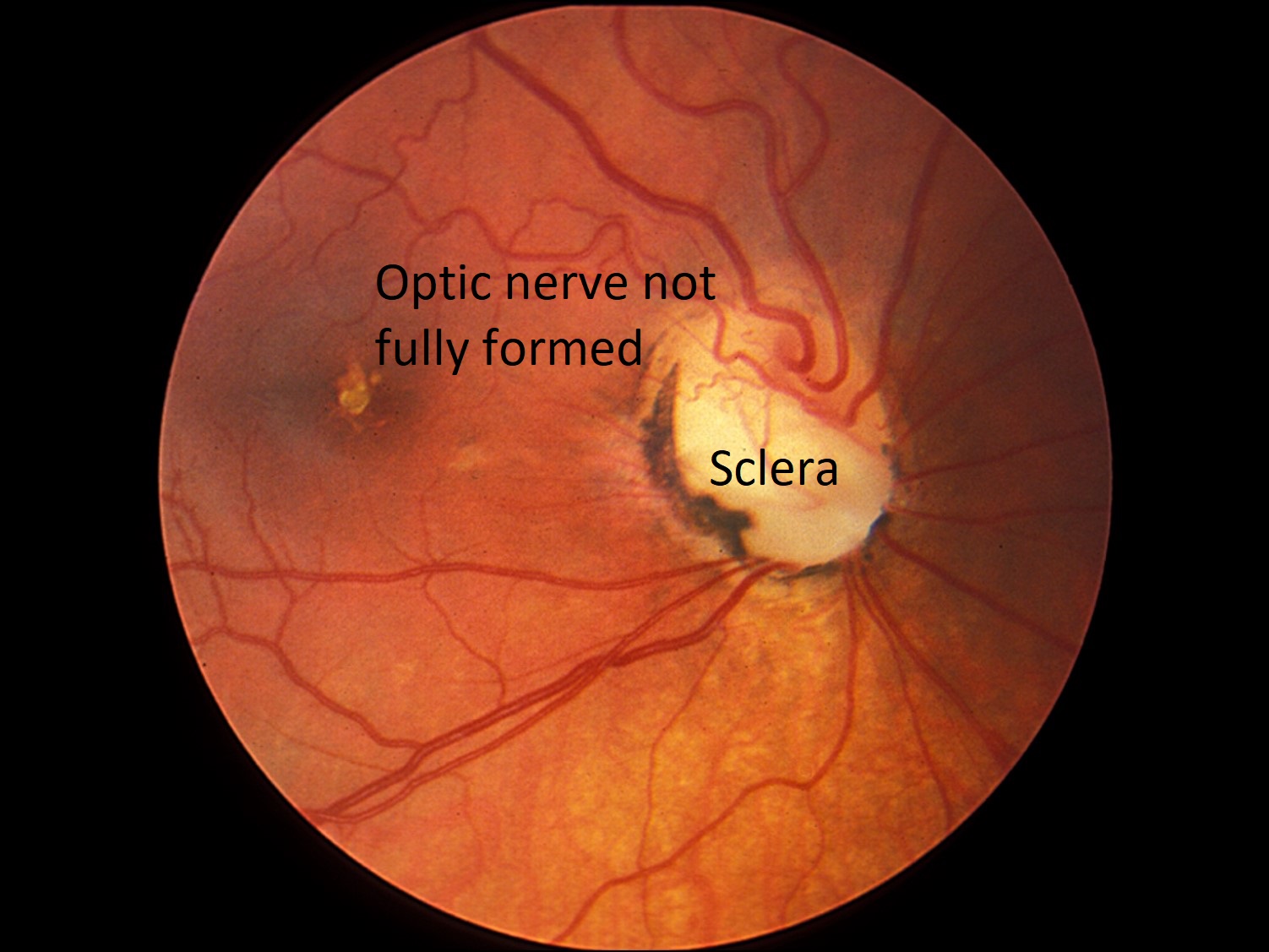
Fundus photo

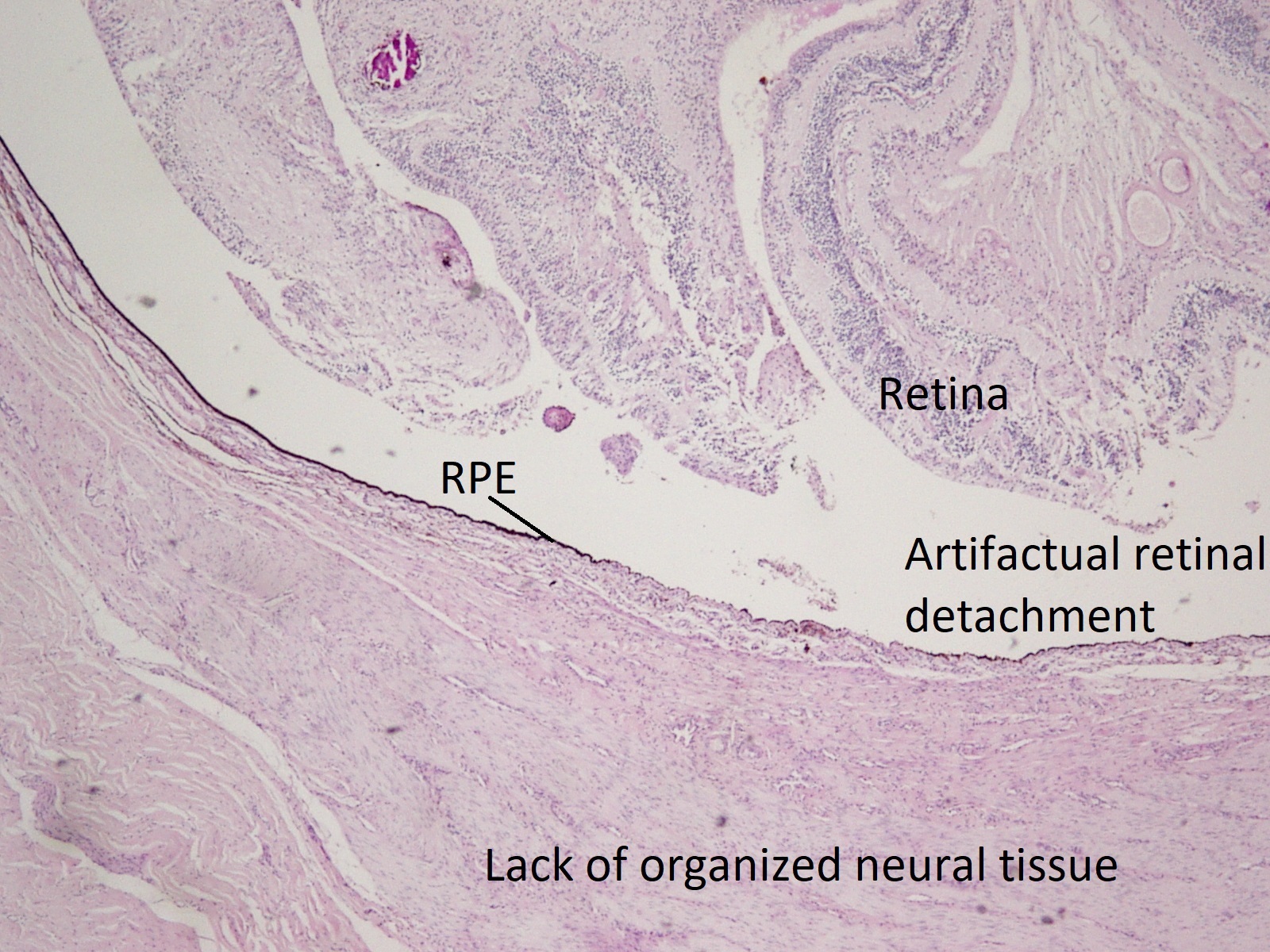
Optic nerve Coloboma PAS stain
- Incomplete closure of the ophthalmic fissure during embryonic development
- Usually located inferonasally on the optic nerve head
- Also associated with colobomas of the retina, choroid, ciliary body, and iris
- If inherited, likely autosomal dominant and bilateral
- Prolapse of disorganized, gliotic retina into the defect noted on histology
- Wall of defectmay contain adipose or smooth muscle
- Normal retina, RPE, and choroid end at the edge of the coloboma
Morning Glory Syndrome

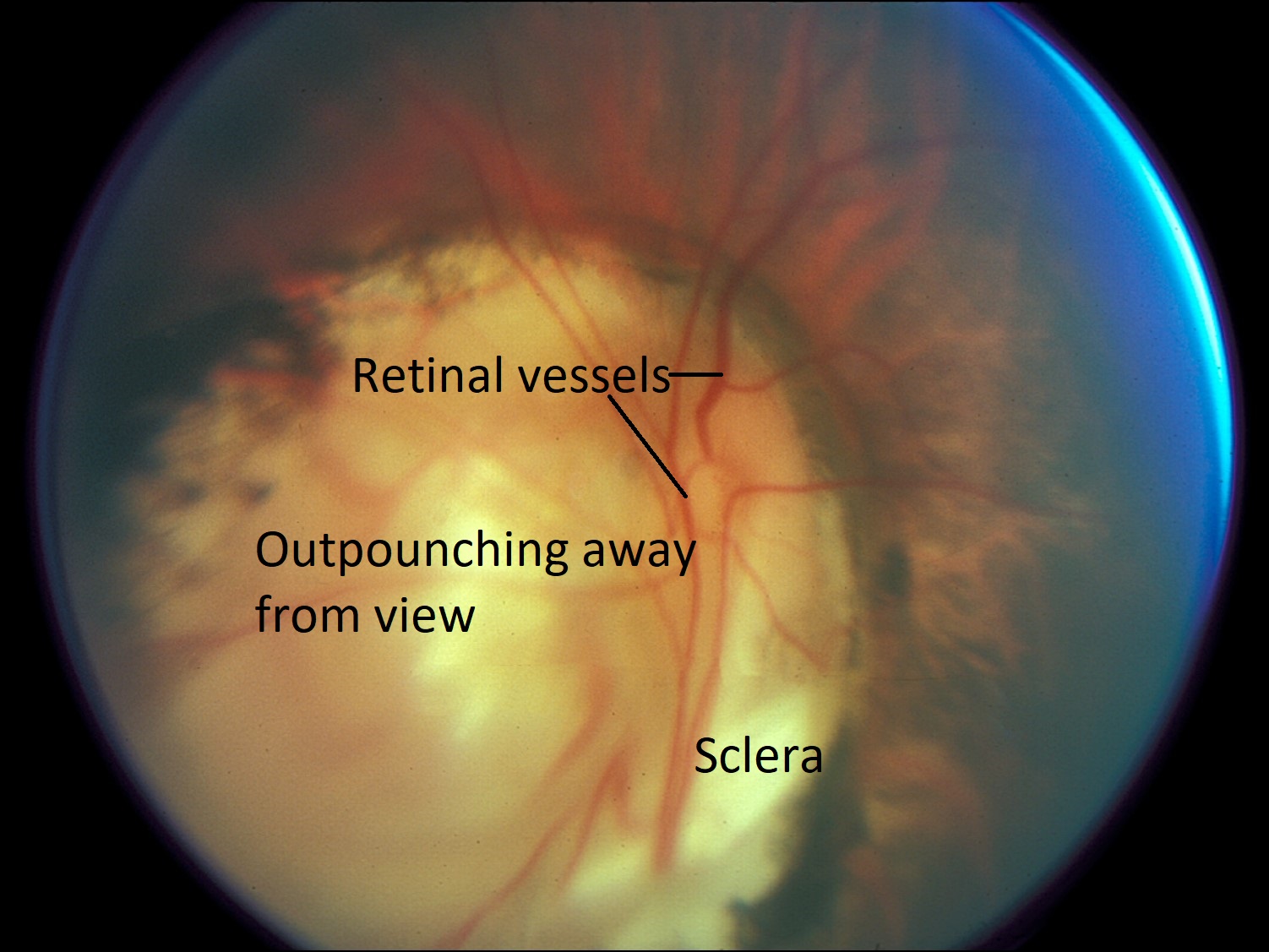
Fundus photo


Morning Glory flower
- Essentially a massive staphyloma around the optic nerve
- Funnel-shaped defect
- Posteriorly displaced optic disc within colobomatous, staphylomatous defect
Optic Nerve Pit

Fundus photo

Optic nerve pit
- Also a defect in closure of the fetal fissure
- Usually located inferotemporally on the optic nerve head
- About 1/8-1/2 optic disc diameter
- Association with visual field defects, serous retinal detachments, and coloboma
- In the location of the pit, there is loss of retinal ganglion cells and nerve fibers.
- Where the optic nerve does not match up with sclera, CSF can flow underneath and reach the macula, causing vision loss.
Optic Nerve Hypoplasia


Fundus photo
- Scleral show with a small optic nerve head
- Whereas scleral show with a large optic nerve head is likely indicative of a myope
- Bilateral
- Inherited, usually autosomal dominant
- Due to abnormal development of retinal ganglion cells
- On histology, partial or total absence of neurons
- Has little effect on vision
Myelinated Nerve Fiber Layer

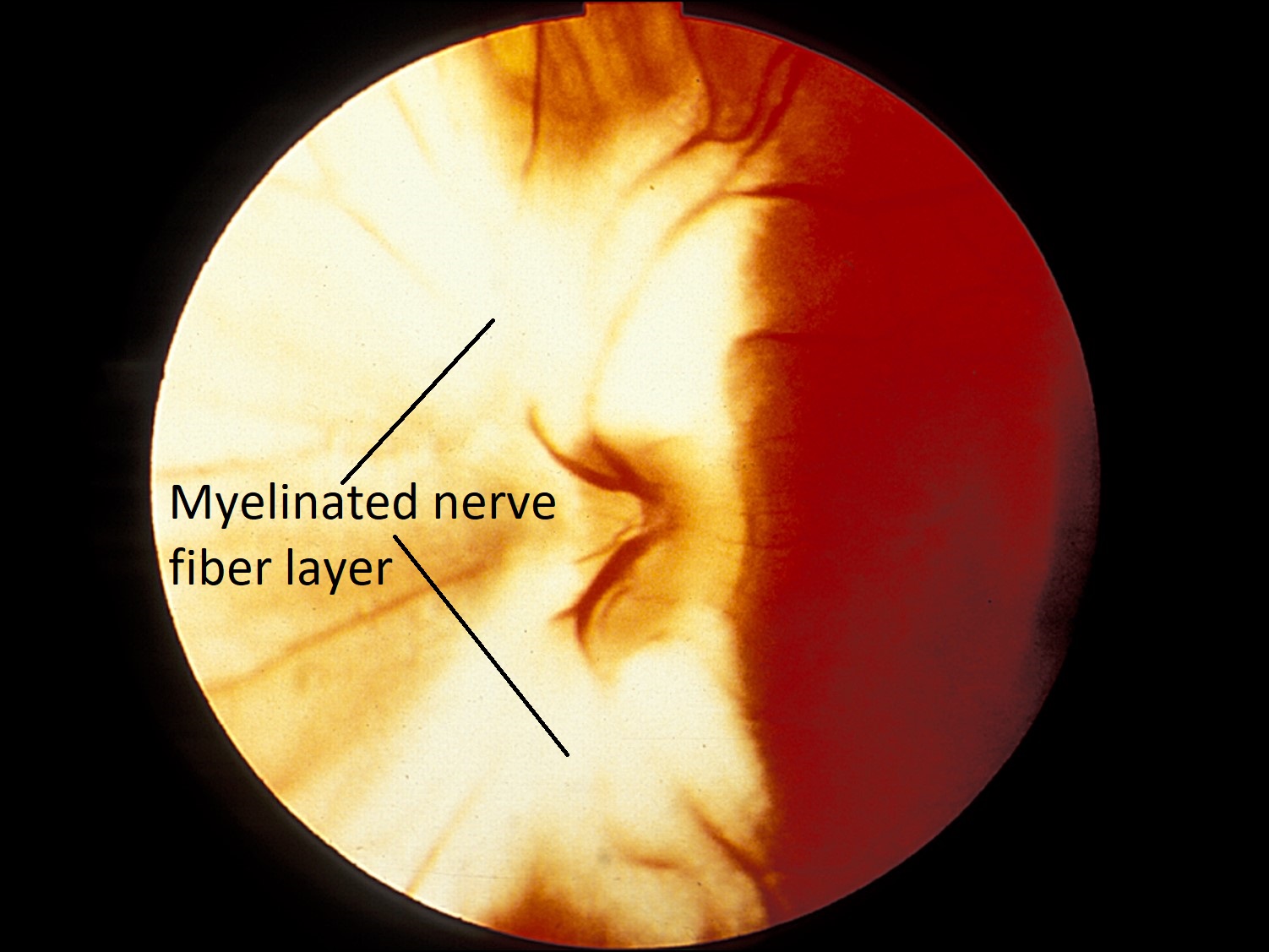
Fundus Photo
- White nerve fibers seen emanating from the disc
- Enlarged blind spot, but vision normal
- Can clinically be confused with optic nerve edema
Optic Nerve Infection (Bacterial, Fungal, Viral)
- Either secondary to extension of bacterial or fungal infection of nearby structures (eye, brain, sinuses) or to a systemic infection (immunosuppressed)
- Fungal
- Mucormycosis: from neighboring sinus infection
- Cryptococcosis: from direct spread of CNS infection
- Multiple necrotic foci with little inflammatory response
- Coccidiomycosis: produce necrotizing granulomas
- Viral: associated with other CNS lesions
- One of the many possible causes of MS and acute disseminated encephalomyelitis
- Macrophages remove damaged myelin
- Glial scar or plaque: result of astrocyte proliferation
- Viral: associated with other CNS lesions
Giant Cell Arteritis
Negative TA Biopsy


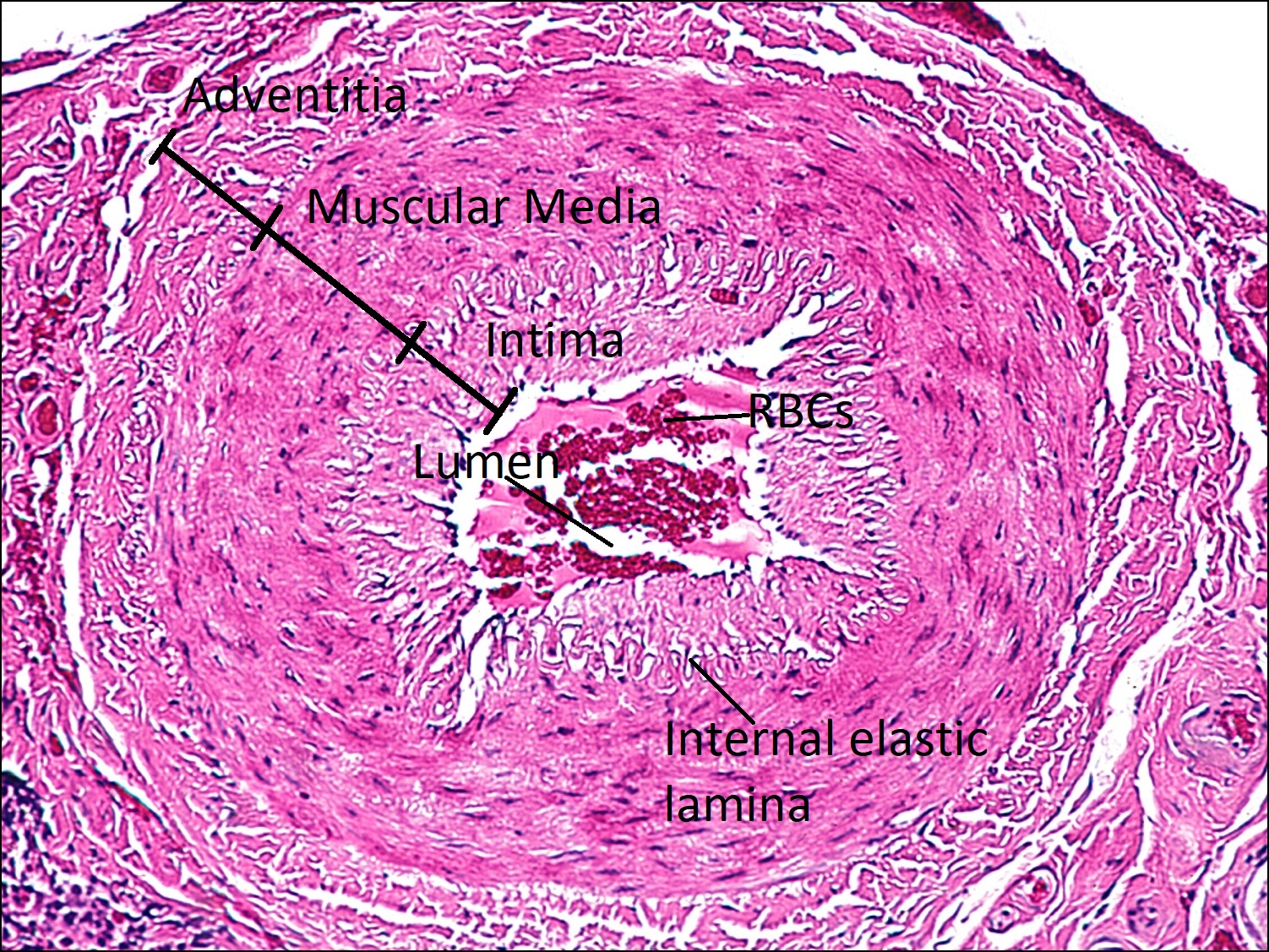
Positive TA Biopsy
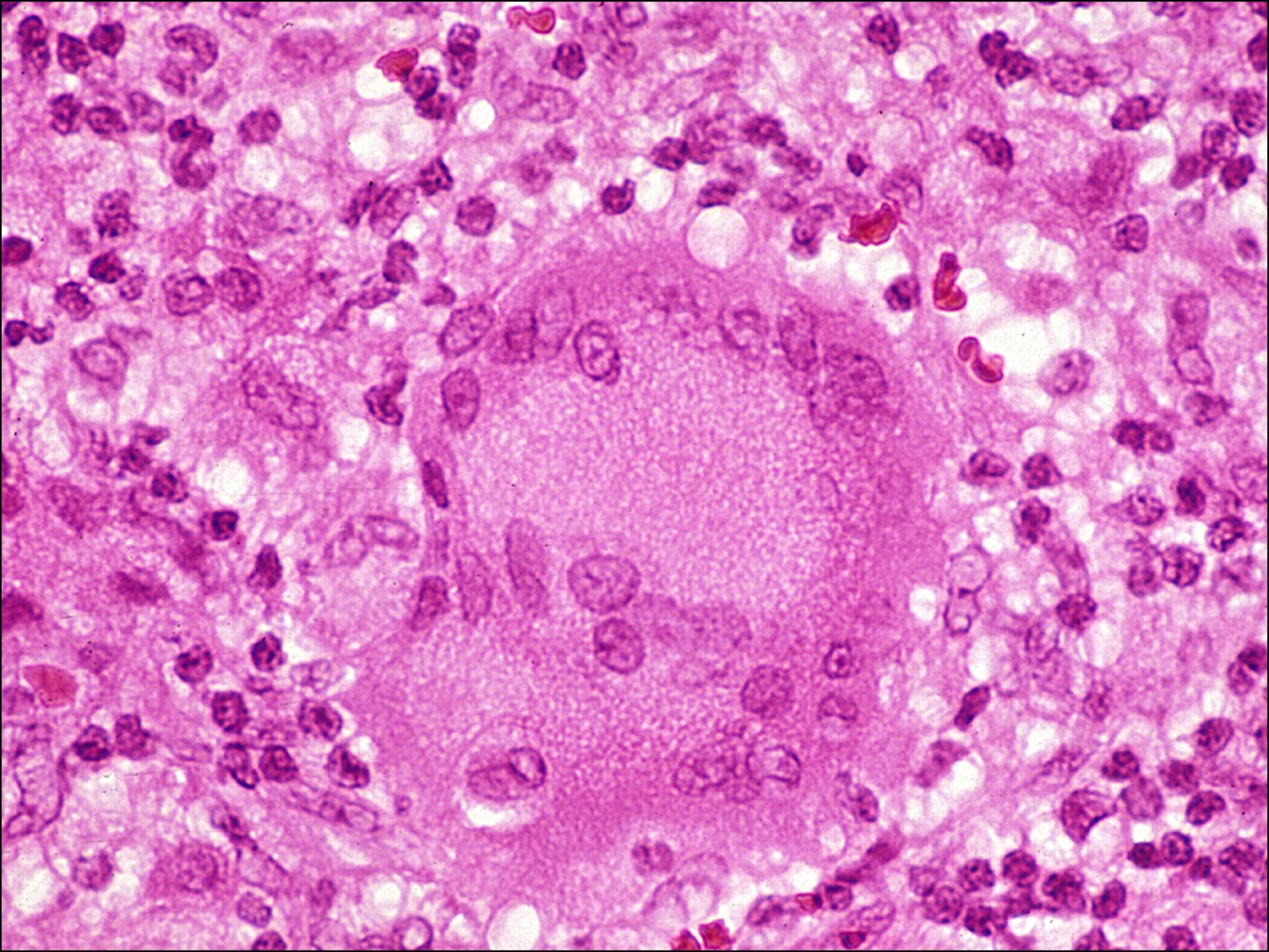

Giant Cell
- Granulomatous inflammation of blood vessel wall
- Most commonly affects middle-aged or elderly women
- Occlusion of posterior ciliary vessels leads to optic nerve necrosis
- AKA Arteritic Anterior Ischemic Optic Neuropathy (AAION)
- Diagnosis: superficial temporal artery biopsy
- Positive Temporal Artery (TA) biopsy
- Disrupted internal elastic lamina
- Abnormal muscular media
- Multinucleated giant cells present
- Surrounding “cuff of blue” lymphocytes in the adventitia
- Intact intima
- A thickened intima is due to atherosclerotic changes
- Occluded lumen


Healed Temporal Arteritis
- Healed temporal arteritis: focally damaged internal elastic lamina and muscular media, but no active inflammatory reaction
- Found if patient has already been treated with steroids when biopsy taken
Sarcoidosis of the Optic Nerve


Noncaseating granuloma
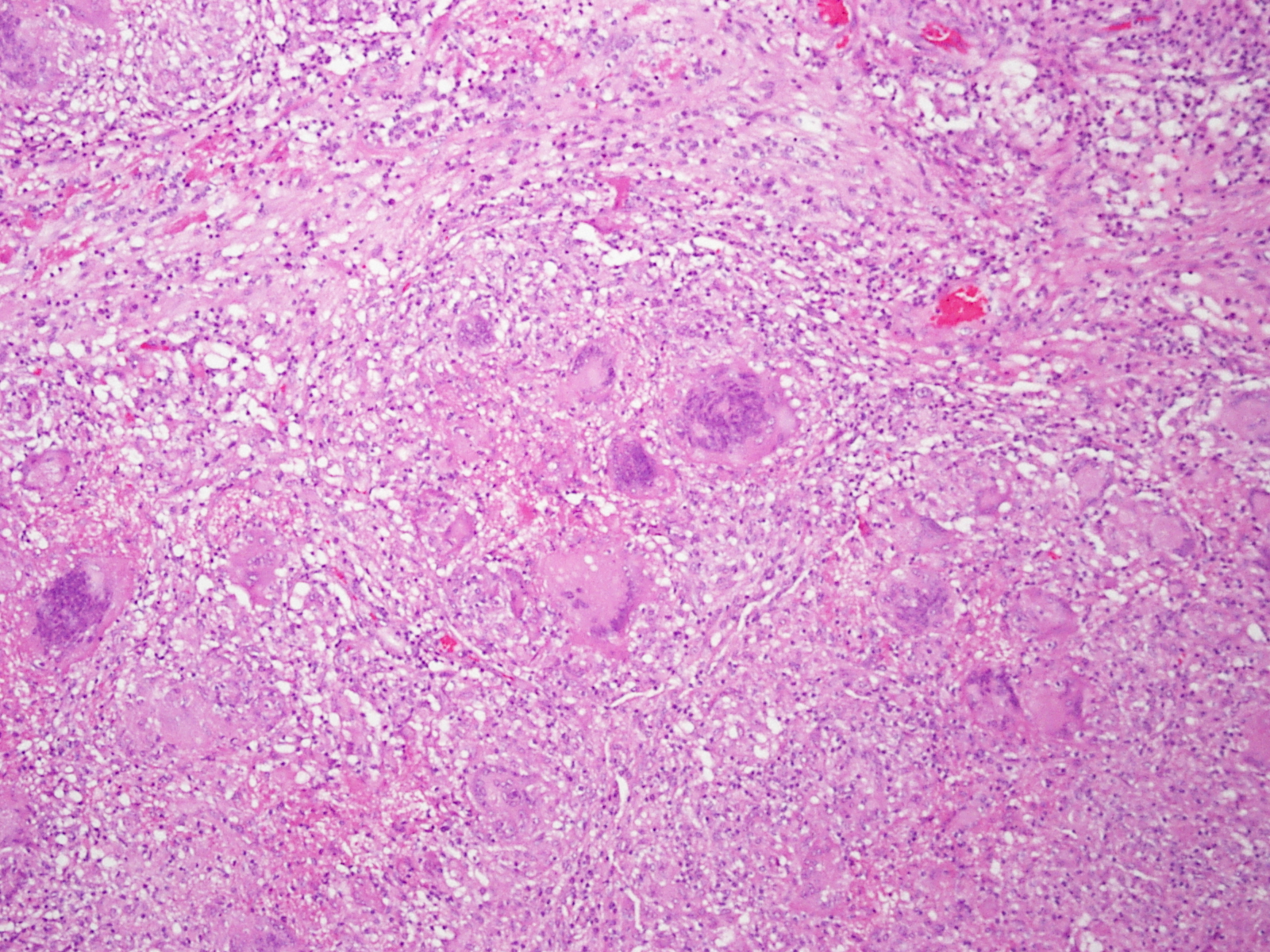

Multinucleated giant cells
- Noncaseating granulomas and possible necrosis of the optic nerve seen
- Multinucleated giant cells in the granulomas
- Associated with retinal, vitreal, and uveitic lesions
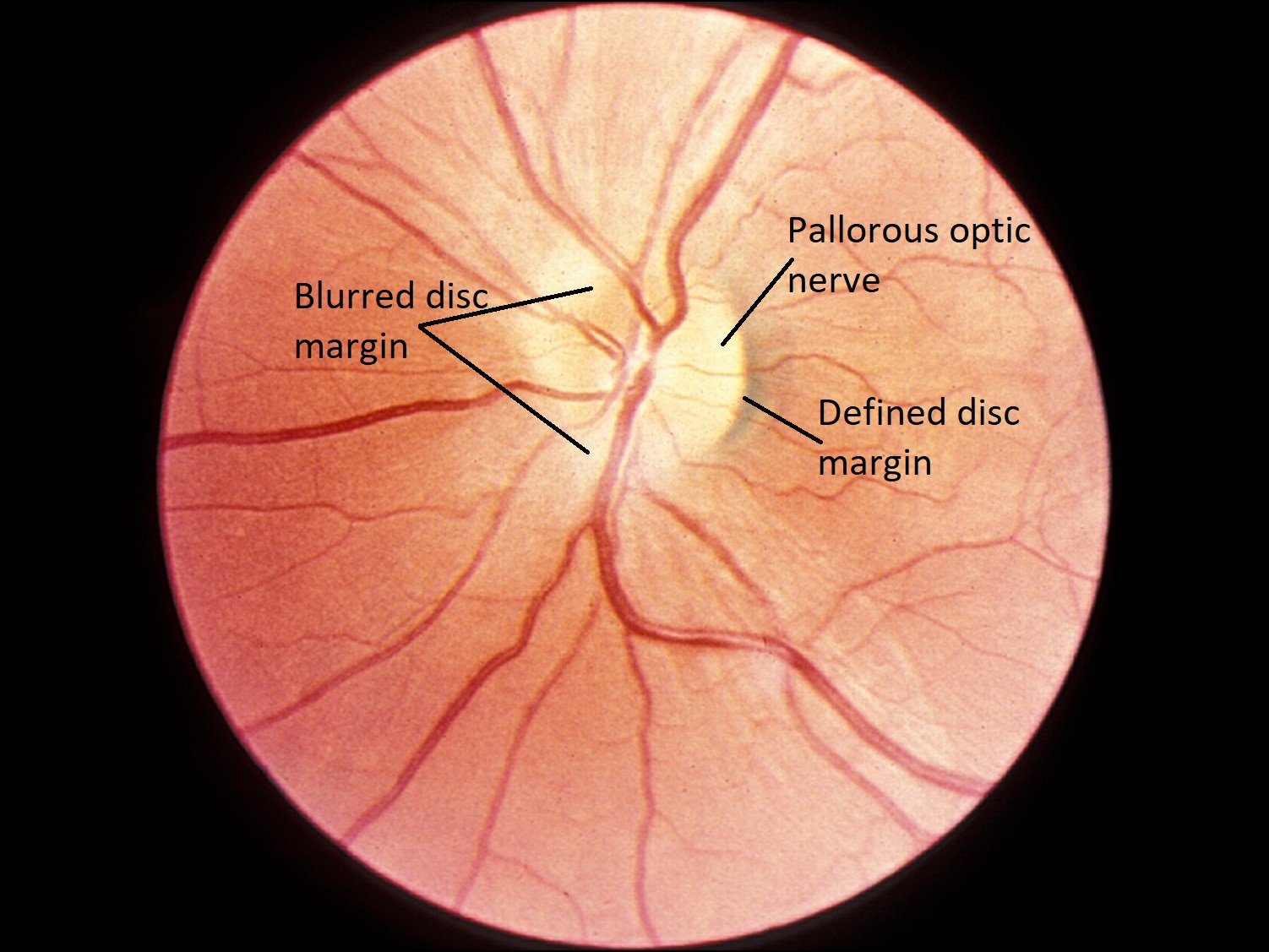
Optic Atrophy
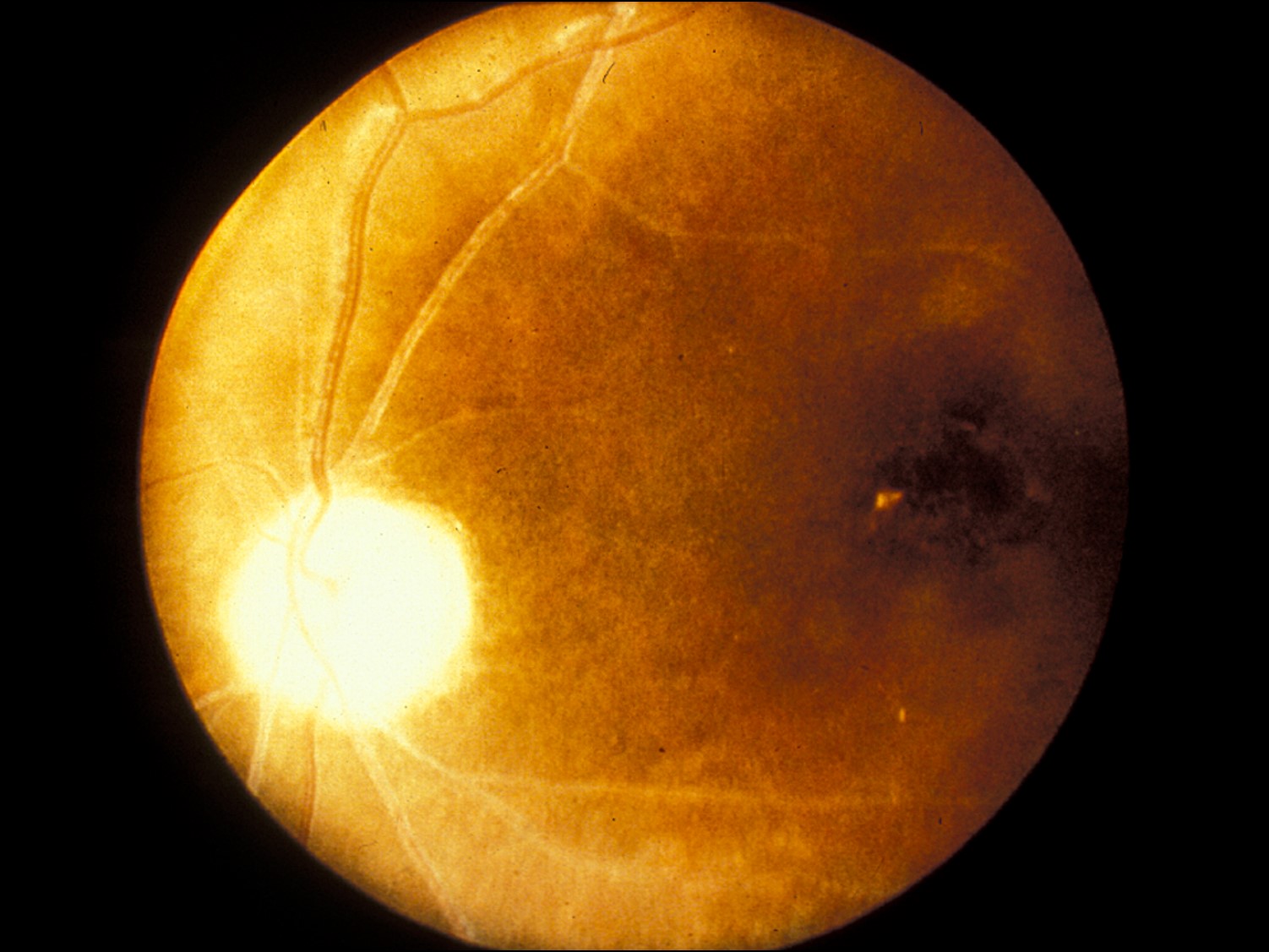

Fundus photo
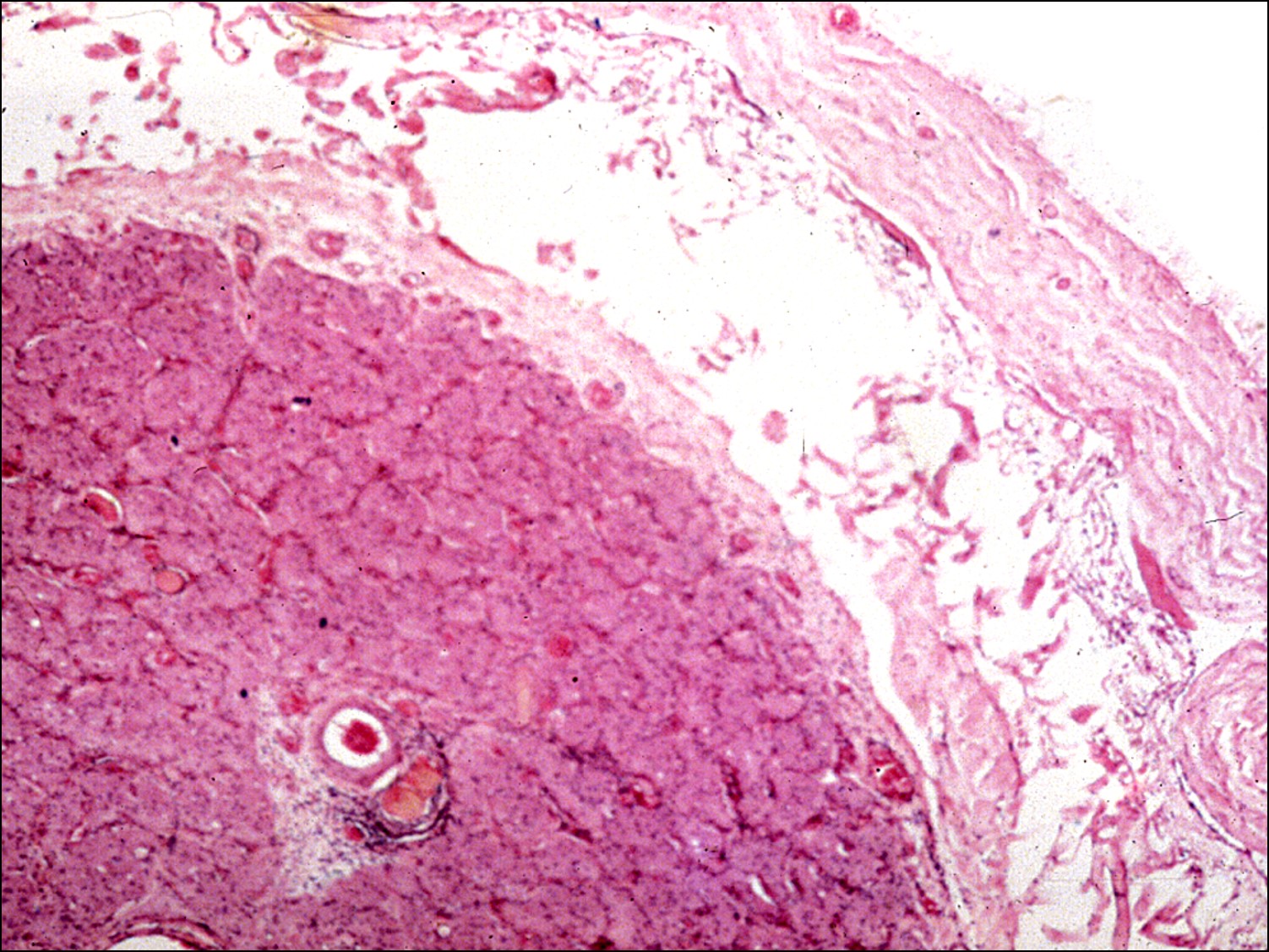
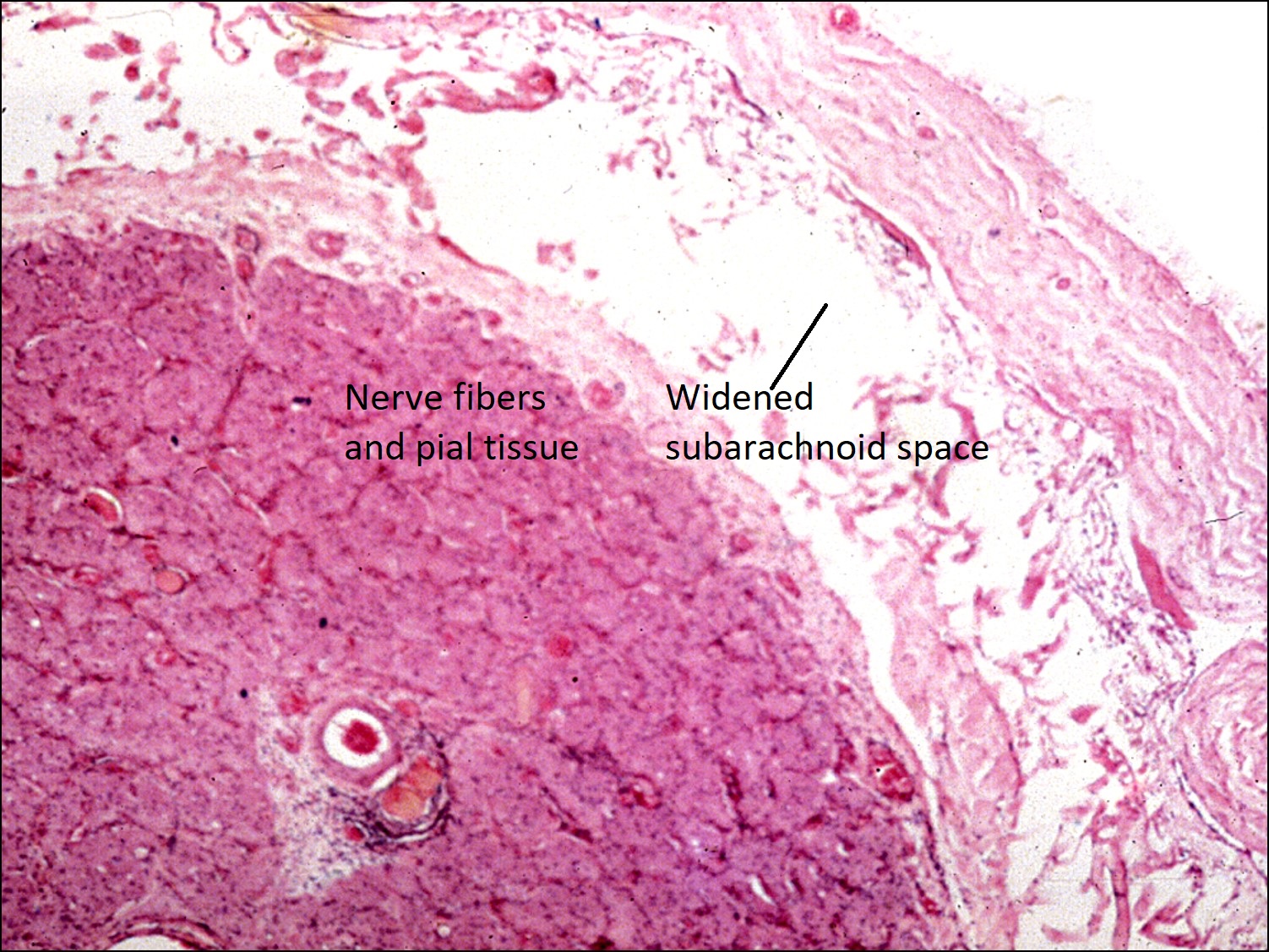
Widened subarachnoid space
- Loss of nerve axons secondary to any cause (ischemia, inflammation, etc)
- Ascending atrophy (Wallerian degeneration): loss of retinal ganglion cells leads to degeneration of axons toward the lateral geniculate body
- Descending atrophy: degeneration of axons toward retinal ganglion cells, due to pathology in cranial cavity or orbit
- Clinical appearance of a pallorous optic nerve
- Loss of myelin and oligodendrocytes
- Optic disc cup deepens, exposing the lamina cribrosa
- Proliferation of astrocytes and pial septa connective tissue
- Widened subarachnoid space from optic nerve shrinkage
- Glaucomatous optic atrophy: high IOP damages optic disc and leads to enlargement of the cup
Nick’s tips: Just because an optic nerve does not clinically appear pallorous or atrophic does not mean that atrophic changes have not already taken place. In ischemic optic neuropathy, it takes weeks to months for the optic nerve to progress to atrophy.
Cavernous Optic Atrophy of Schnabel


Cystic atrophy
- Cystic atrophy of the optic nerve posterior to the lamina cribrosa
- Cysts filled with mucopolysaccharide and stains with Alcian blue
- Mucopolysaccharide material likely produced within the atrophic areas of the nerve
- Initially noted in glaucomatous eyes following acute IOP increase
- Also seen in nonglaucomatous elderly eyes with systemic arteriosclerosis
Optic Nerve Drusen


Buried drusen

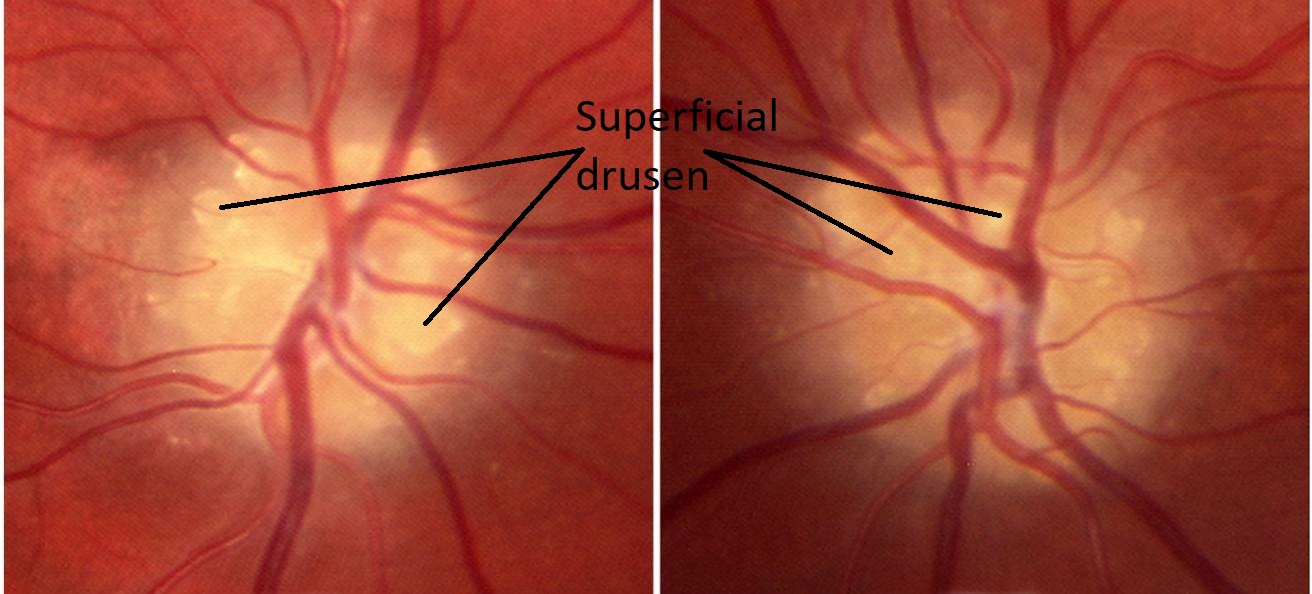
Superficial drusen


Optic nerve drusen


Deep drusen resembling edema


CT scan showing drusen


Gross photo of sagittal cut

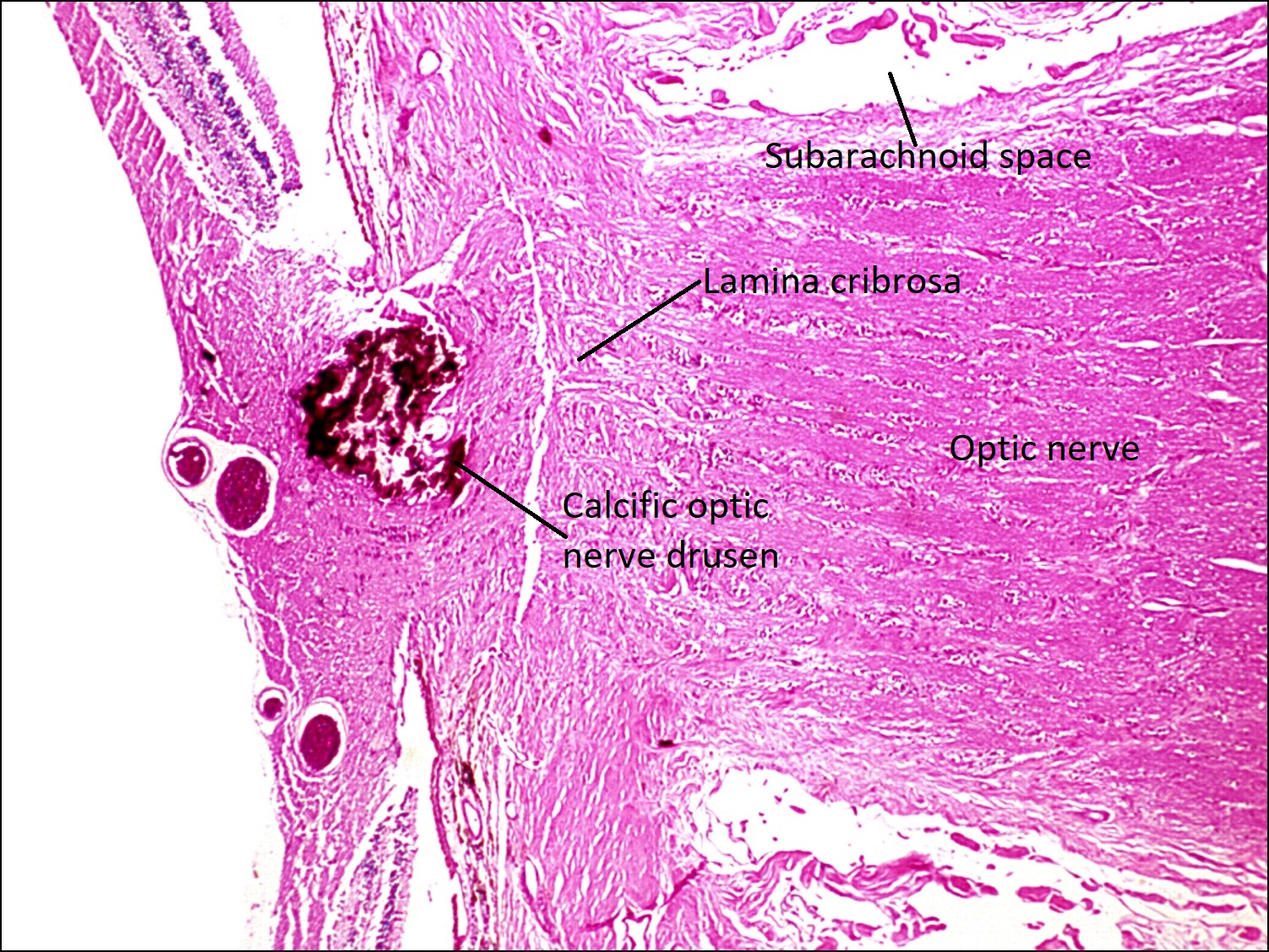
Anterior to lamina cribrosa

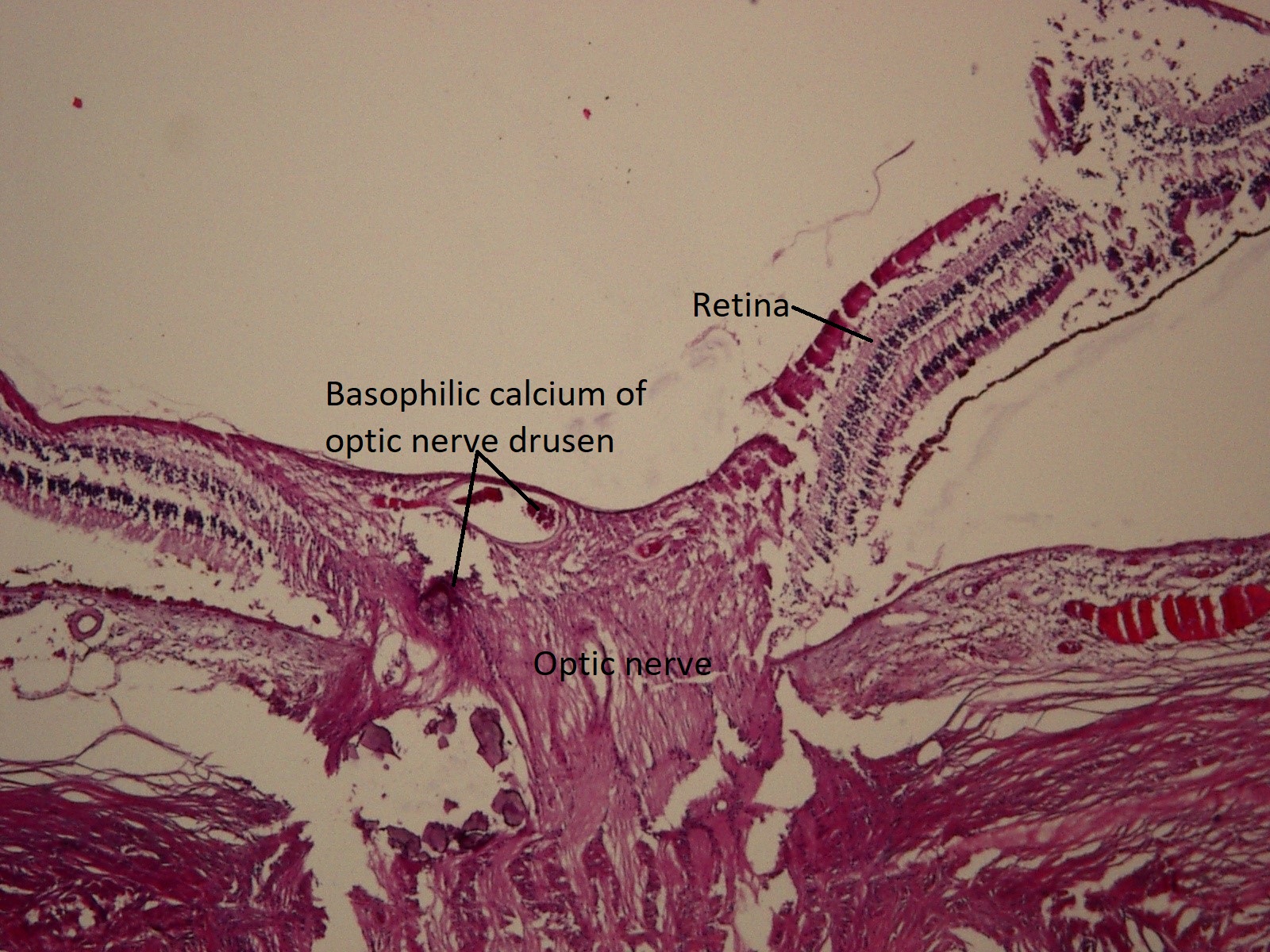
Basophilic-staining calcium deposits
- Calcified and hyalinized deposits anterior to lamina cribrosa
- Superficial drusen appear refractile, round, and pale yellow or white
- Deep drusen can be mistaken for papilledema, therefore pseudopapilledema
- No engorged vessels or hemorrhages like would be seen in optic disc edema
- Bilateral
- Sometimes inherited
- Found in small, crowded optic discs
- Basophilic acellular calcified deposits located anterior to lamina cribrosa and posterior to Bruch’s membrane
- Association with angioid streaks, papillitis, optic atrophy, chronic glaucoma, and vascular occlusions
- More common in normal eyes
- As drusen enlarge, they can impinge on the nerve fiber layer and cause focal defects
- Diagnosis: appear as white foci on B-scan and CT scan
- Inconsistently shows up on autofluorescence
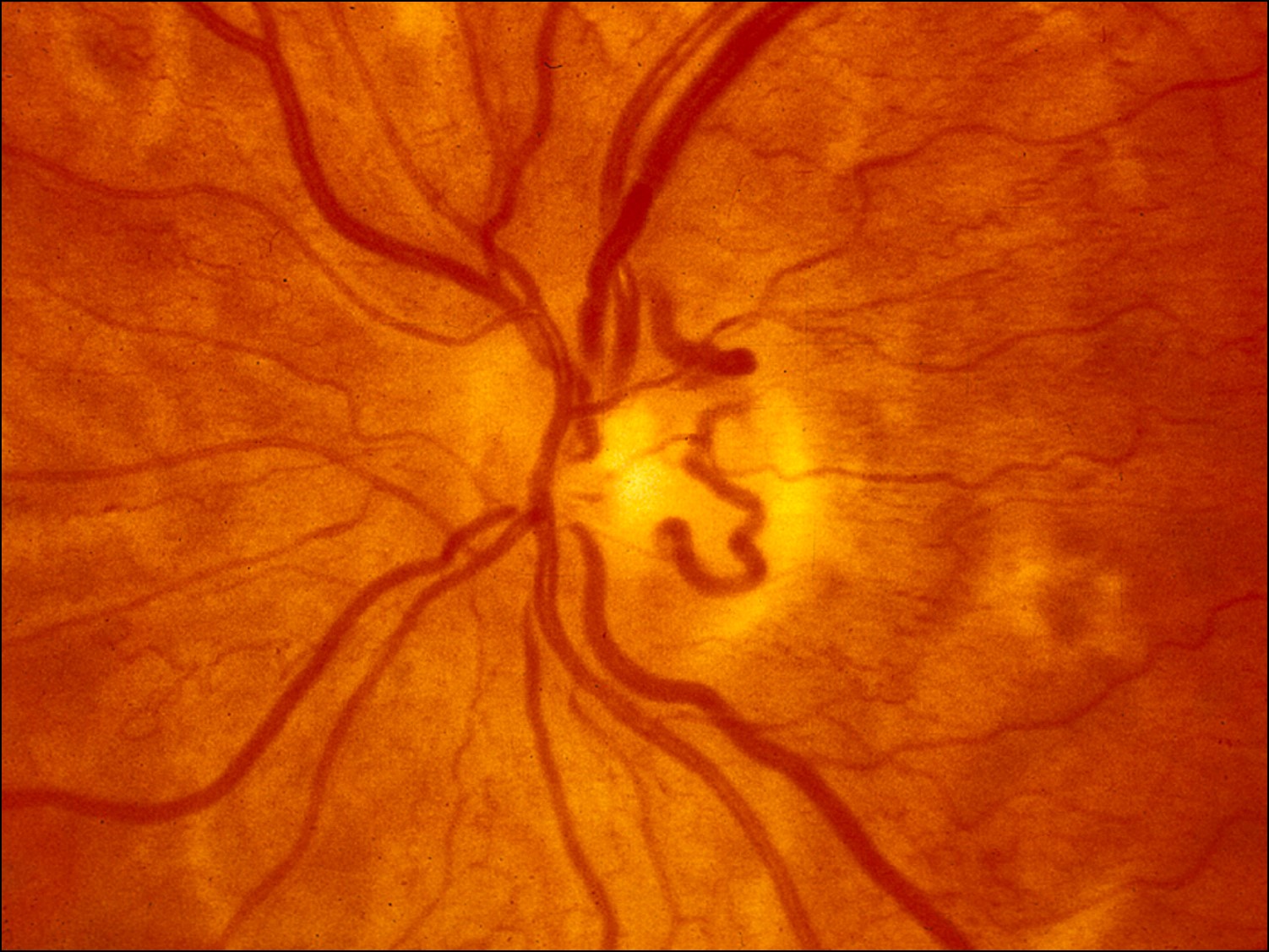
Optic Nerve Edema

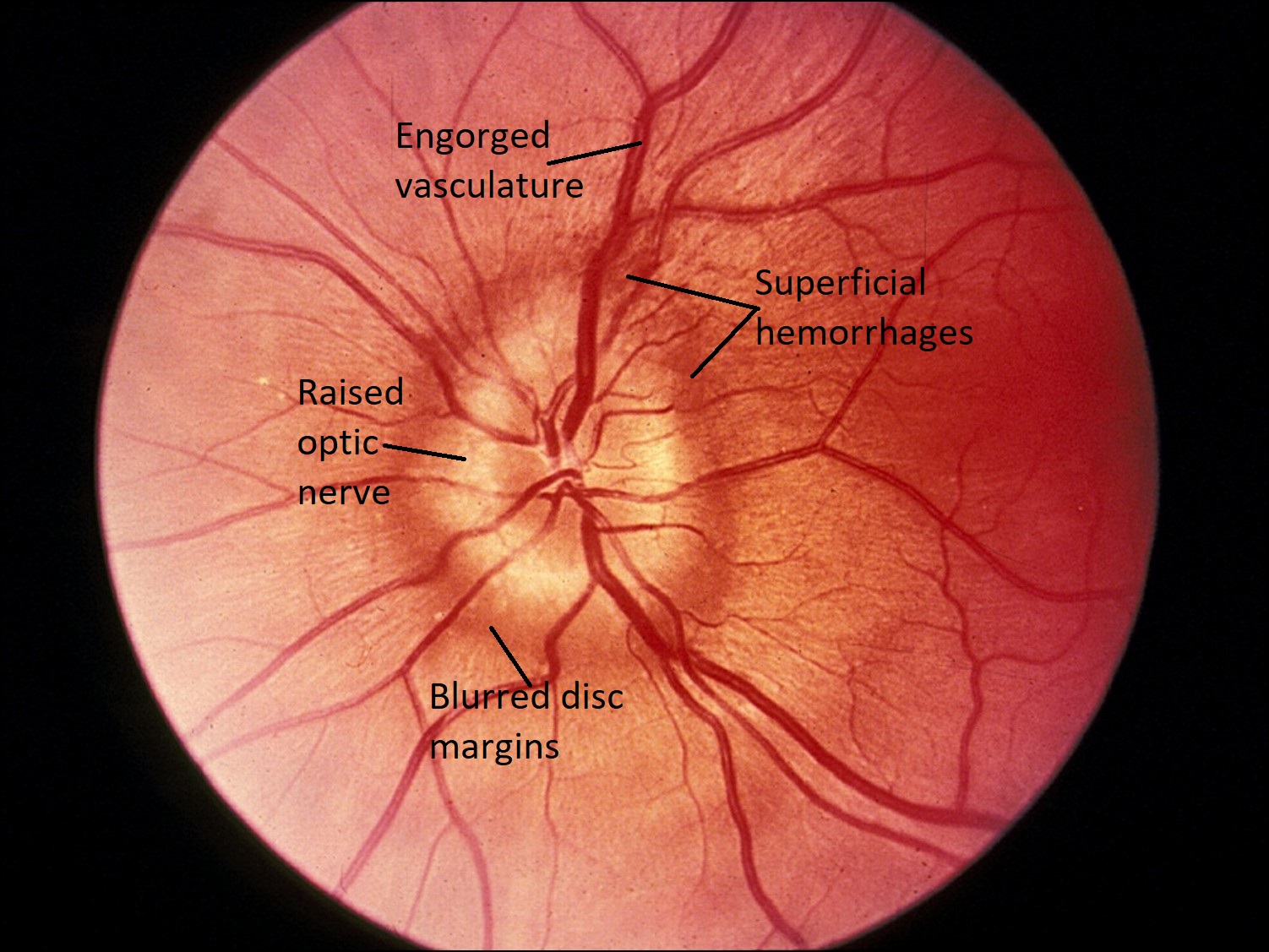
Fundus photo

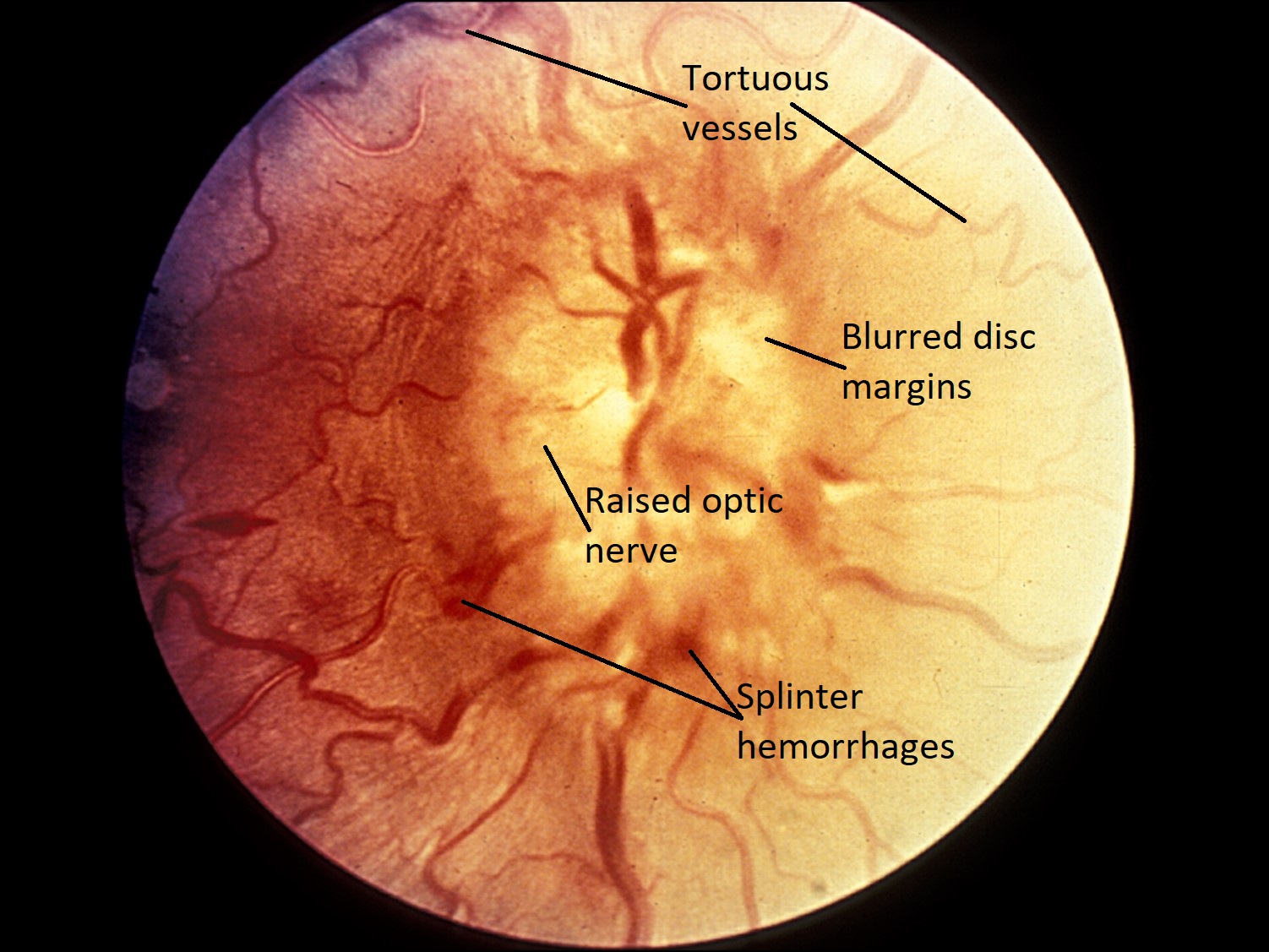
Tortuous vessels


Anterior bowing of lamina

Optic nerve edema
- Raised optic nerve with blurred disc margins
- Enlarged blind spot, but normal vision
- Engorged vasculature and splinter hemorrhages
- Histologically, can see forward bowing of the lamina cribrosa and swelling of the optic nerve
- Absent optic cup
- Vascular congestion and superficial hemorrhages may be present
- Papilledema: bilateral optic nerve edema secondary to increased intracranial pressure
- If untreated, can lead to peripheral vision loss that progresses to the central vision
- Idiopathic Intracranial Hypertension (IIH) or Pseudotumor Cerebri: increased intracranial pressure without a known cause
- If chronic, can lead to papilledema

Sectoral disc edema
- Differential diagnosis for sectoral disc edema: non-arteritic anterior ischemic optic neuropathy (NAION), arteritic anterior ischemic optic neuropathy (Giant Cell Arteritis), optic neuritis
- Focal areas of axonal loss
- NAION: noninflammatory optic disc edema seen in patients usually age 55-70
- Sudden onset of monocular vision loss with altitudinal visual field defect
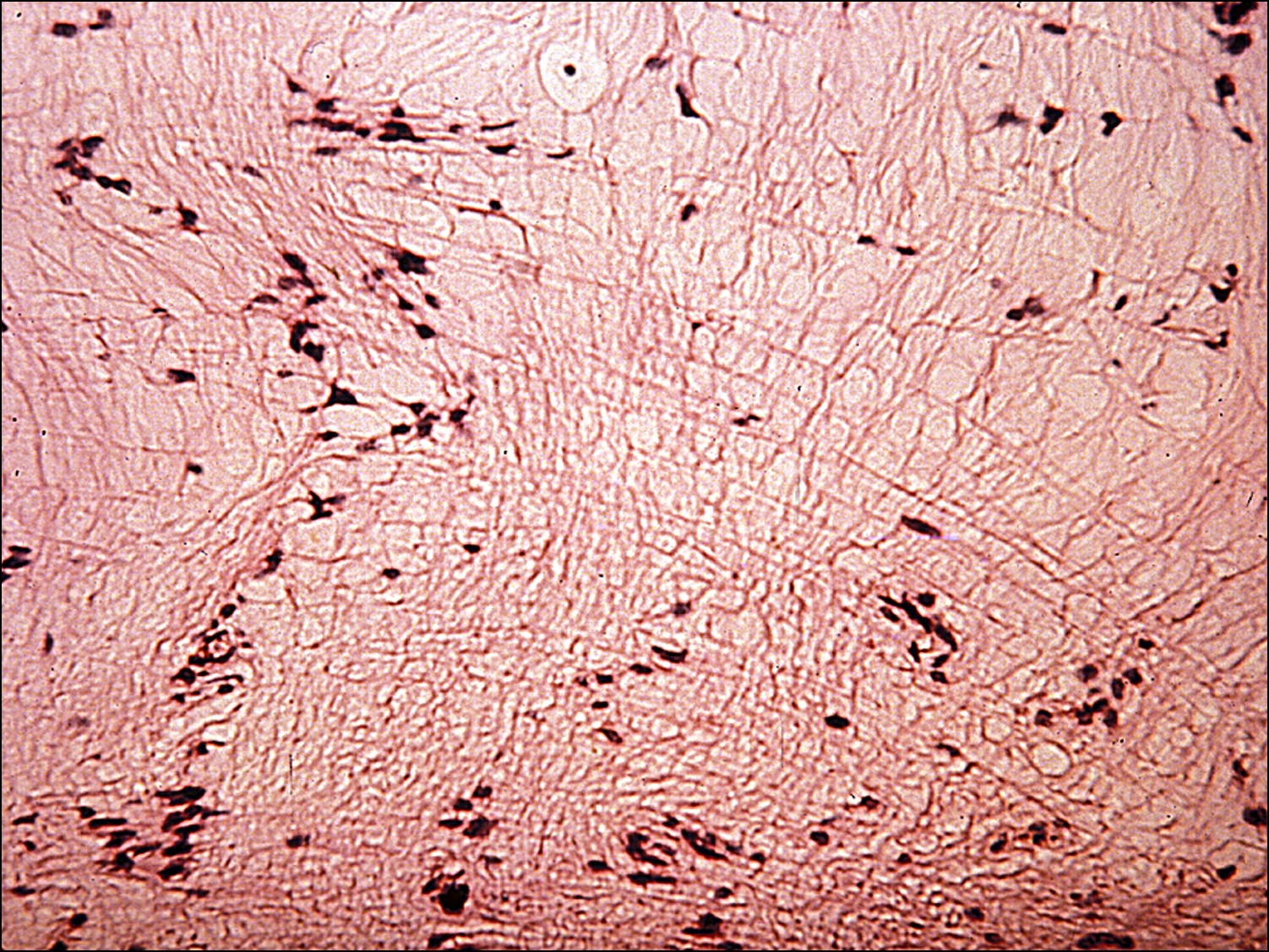
Optic Neuritis


Optic Neuritis

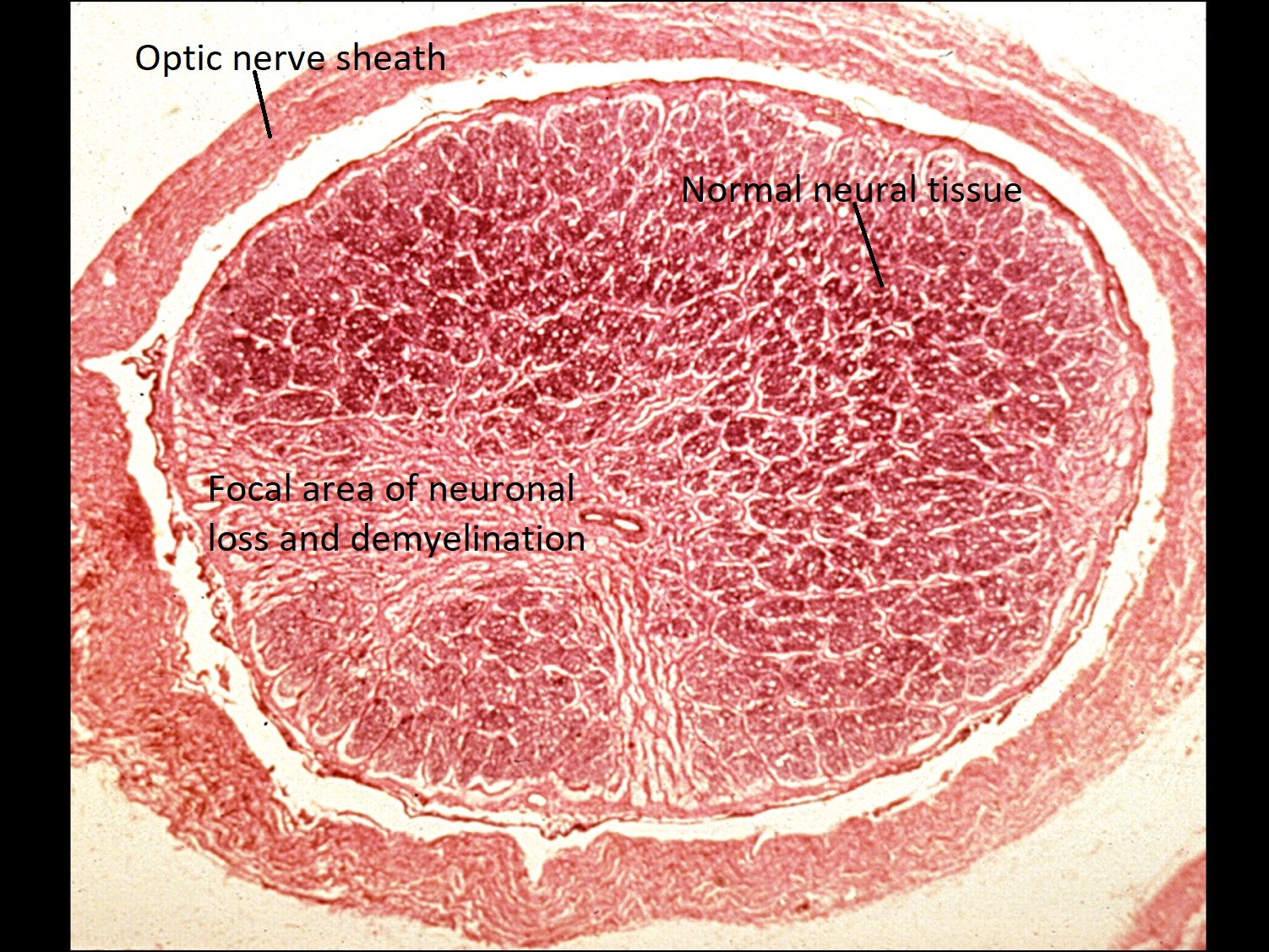
Demyelination
Focal neuronal loss
- Focal neuronal loss with demyelination
- Affects younger patients
- Concern for multiple sclerosis
- Treat with IV steroid taper
- At 6 months, steroid treatment decreases likelihood of or prolongs progression to multiple sclerosis.
Melanocytoma
- Benign, deeply pigmented tumor of the optic disc, anterior to the lamina cribrosa
- Slightly raised, and typically found eccentrically on the optic disc
- Can extend into the retina or posteriorly to the lamina and into the optic nerve
- Rarely becomes malignant
- Essentially a nevus of the optic disc
- Plump, darkly pigmented, densely packed melanocytes
- Melanocytoma cells: plenty of cytoplasm, small nuclei, small and regular nucleoli
- Presence of necrosis or melanophagic infiltrate does not necessarily indicate malignant transformation
Nick’s tips: The dark pigmentation of a melanocytoma often obscures the nuclear details needed to determine atypia. A bleached preparation of the specimen is necessary to observe cytologic features.
Optic Nerve Glioma


External photo

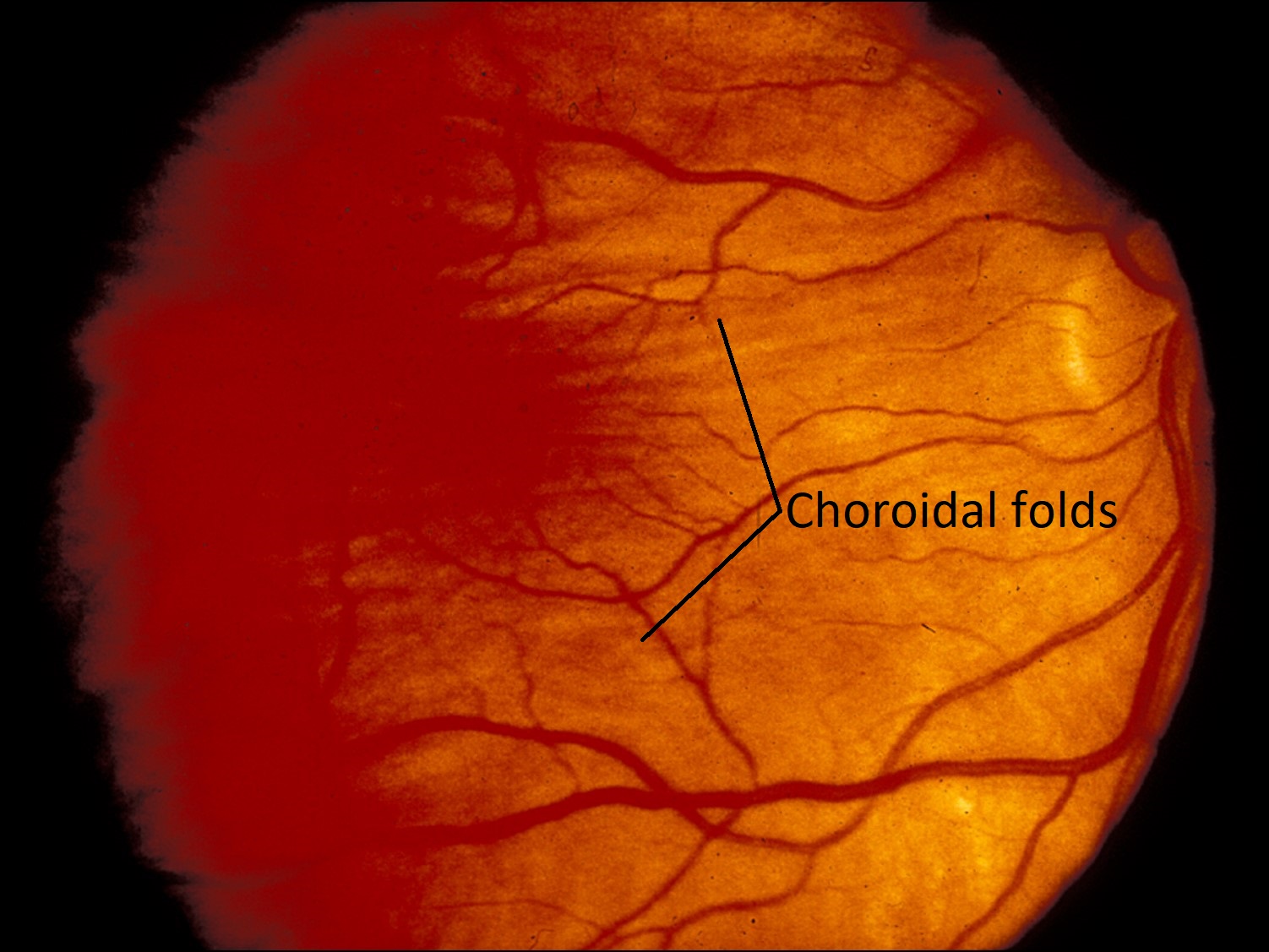
Choroidal folds
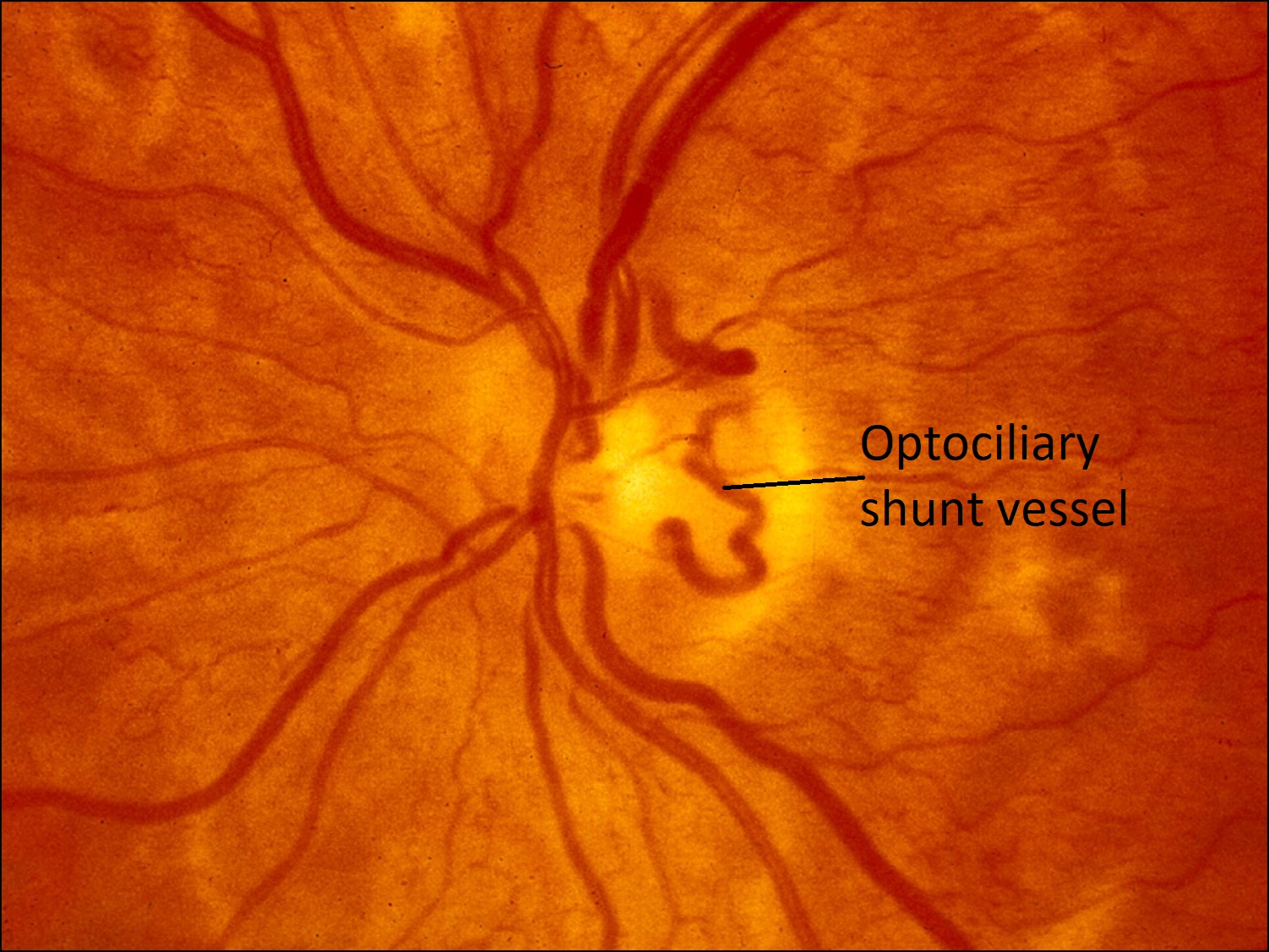
Optociliary shunt vessel
- Optic nerve tumor originating from astrocytes
- Signs of an intraconal tumor
- Proptosis
- Choroidal folds seen on fundus exam
- Optociliary shunt vessels present (general sign of chronic nerve ischemia) on atrophic optic nerve
- More commonly found in young patients within the first decade of life
- If found outside of this typical age group, tumor is more likely to be aggressive


Fusiform mass on CT scan
- CT scan: fusiform mass that is indistinguishable from the optic nerve
- The tumor is contained within the optic nerve sheath


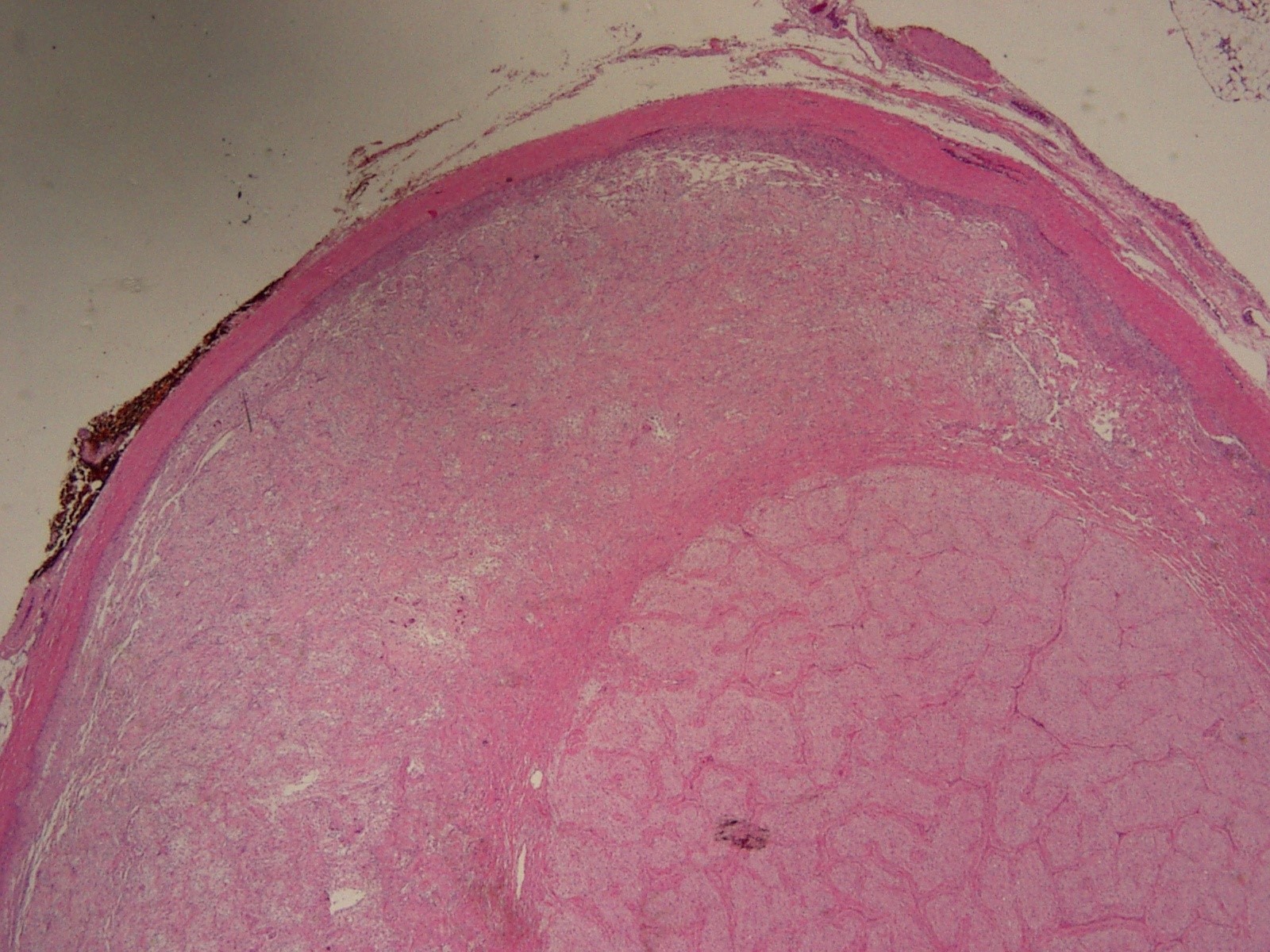
Tumor within optic nerve sheath


Gross photo with attached globe

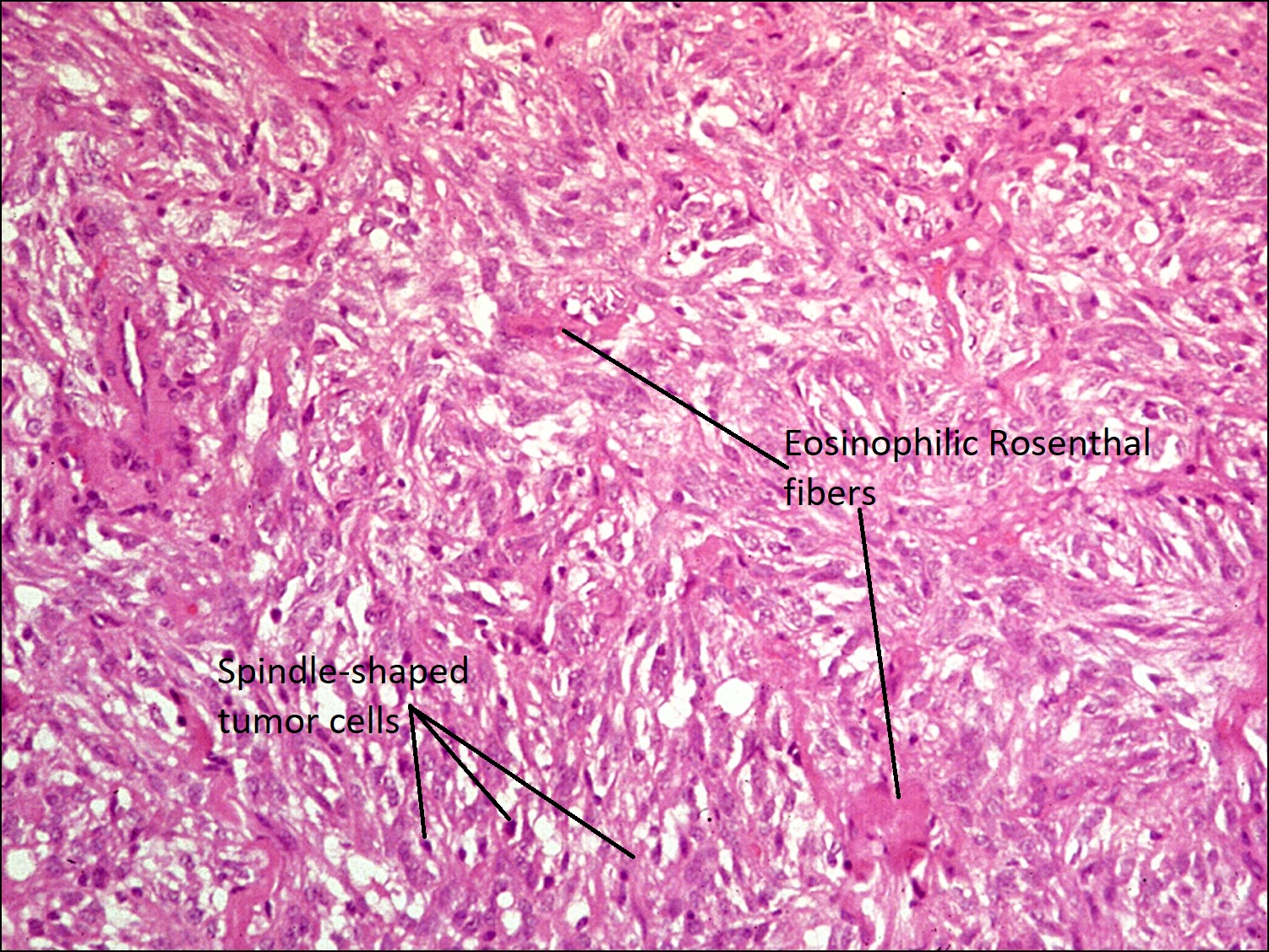
Optic nerve glioma


Microcystic degeneration


Rosenthal fibers

Glioma with normal nerve tissue
- Histology:
- Spindle-shaped or “hair-like” tumor cells without mitotic figures
- Characteristic eosinophilic Rosenthal fibers (cytoplasmic inclusions of degenerating cell components)
- Focal microcystic degeneration, necrosis,and calcification may be present
- Thickened pial septae and disorganized glial nuclei
- Low-grade or Grade I astrocytoma
- AKA Juvenile pilocytic astrocytomas
- High-grade astrocytomas rarely involve optic nerve and, if they do, are usually secondary to a brain tumor
- Primary malignant glioma: affects mostly adults and cells show marked anaplasia, pleomorphism, mitotic activity, necrosis, and hemorrhage
- Association with Neurofibromatosis 1(NF1)
- Treatment strategies do not save the vision
- Can excise the nerve, but the vision is lost
- Can do radiation therapy, which will slow tumor growth, but does not bring back vision that has already been lost.
- Prognosis
- Excellent if astrocytoma limited to orbital optic nerve
- Guarded if intracranial optic nerve involved


Reactive changes of meninges


Meningeal proliferation
Nick’s tips: Oftentimes, the meninges undergo reactive proliferative changes that create structures that resemble psammoma bodies. This is especially tricky if, when taking a biopsy of the optic nerve, the specimen is very superficial and only contains a part of the meninges and no nerve fibers.
Optic Nerve Meningioma


External photo

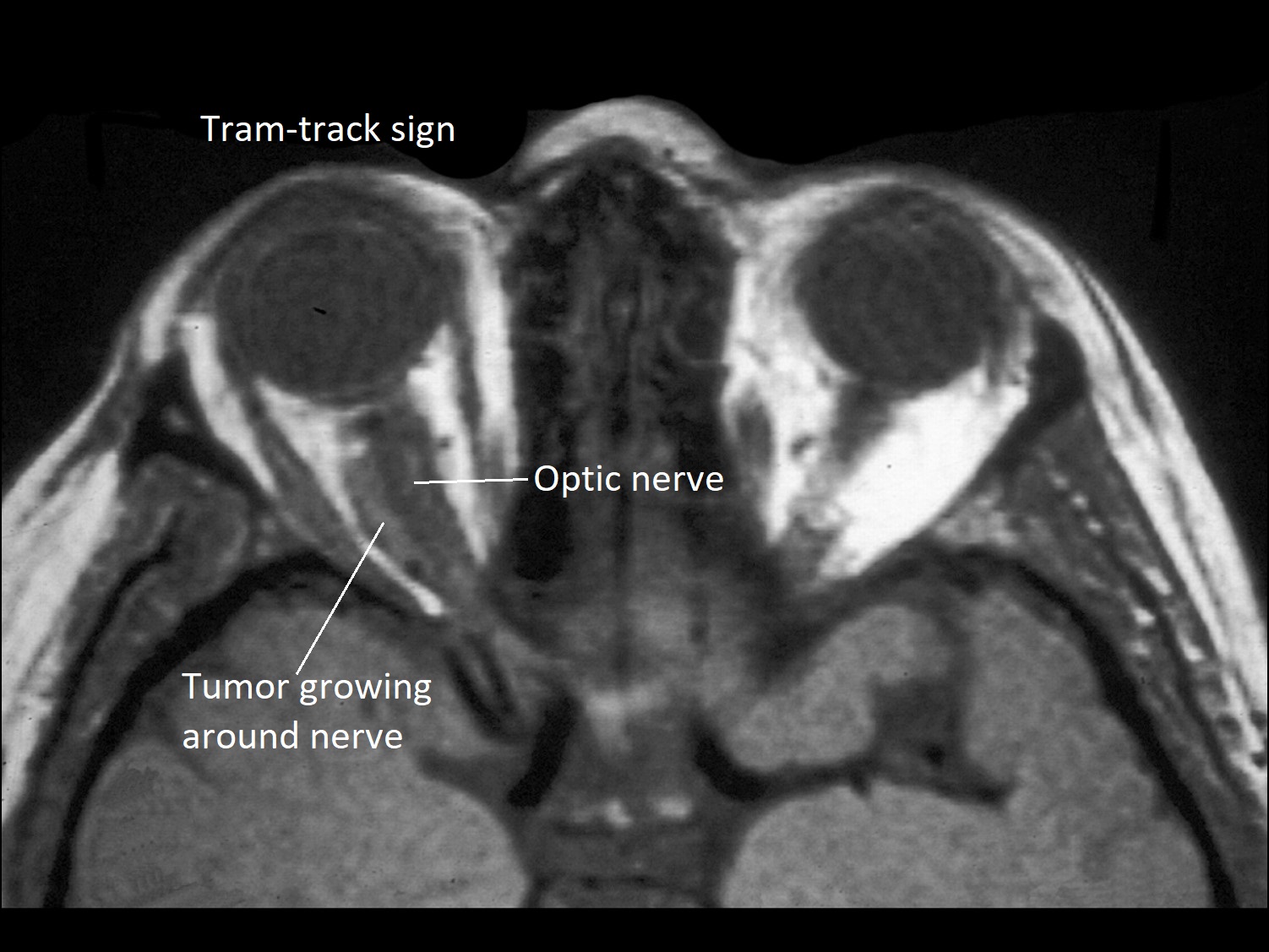
Tram-Track sign on CT scan
- Intraconal tumor originating from the arachnoid sheath
- Less common than a secondary orbital meningioma extending from an intracranial origin
- More commonly found in elderly patients
- If found outside of this typical age group, tumor is more likely to be aggressive
- CT scan: tumor seen growing around optic nerve with Tram-track sign


Gross photo


Meningothelial type


Optic Nerve Meningioma
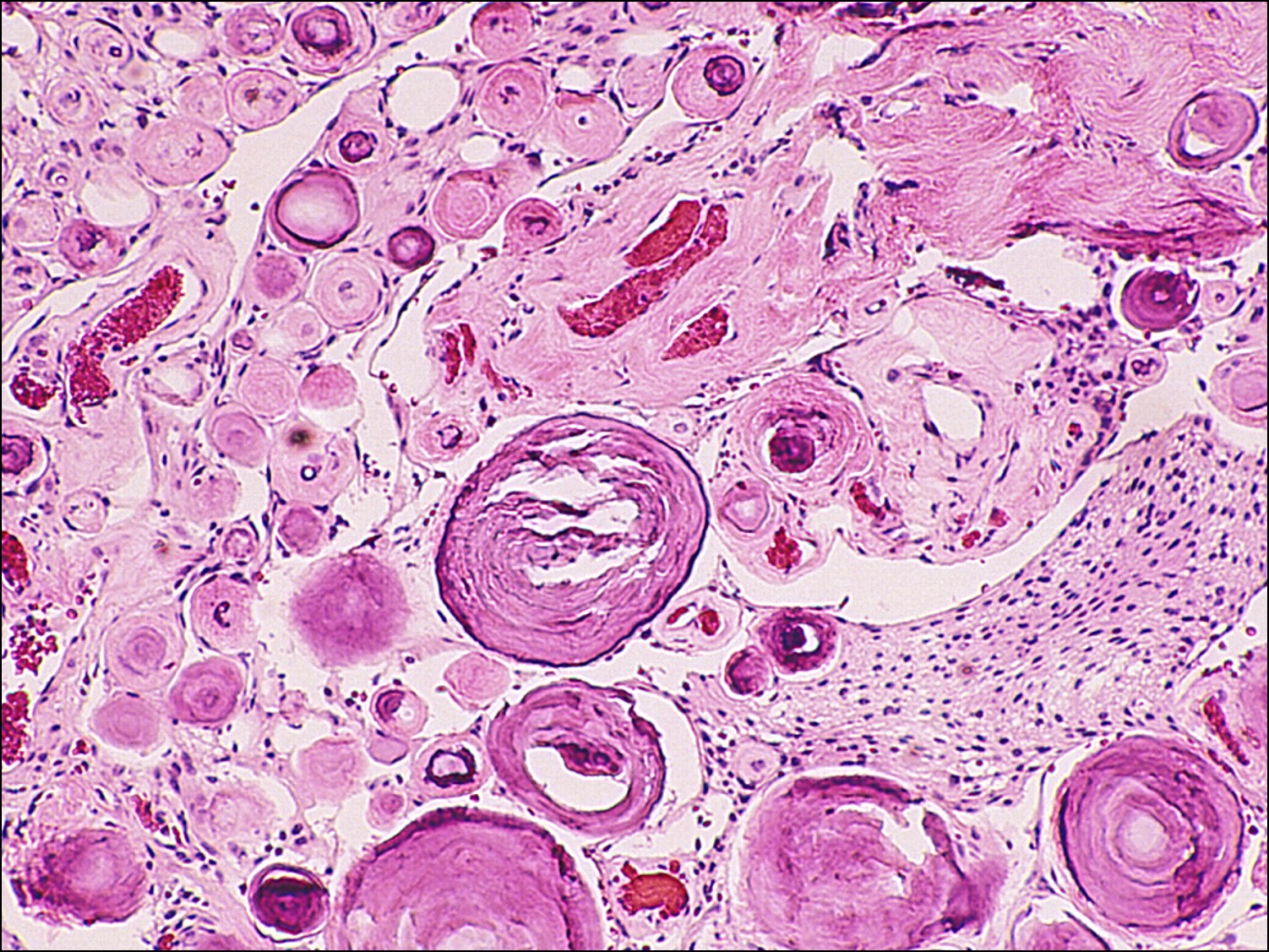

Psammoma bodies
- Histology:
- Meningothelial type: most common histologic variant, whorls of tumor cells seen
- Psammoma bodies: lamellar, hyalinized, calcific, extracellular bodies surrounded by meningioma cells
- Can extend through the optic nerve sheath and into muscleand other orbital tissue or into the nerve and sclera (uncommon)
- In younger patients, may be rarely associated with Neurofibromatosis 1(NF1)
- Looser association with NF1 than optic nerve glioma
- Treatment: peel meninges off the optic nerve, but may damage the blood supply to the nerve in the process, thus ultimately killing the optic nerve
- Prognosis worsens with younger age of onset
Optic Nerve Schwannoma


CT scan of intraconal mass

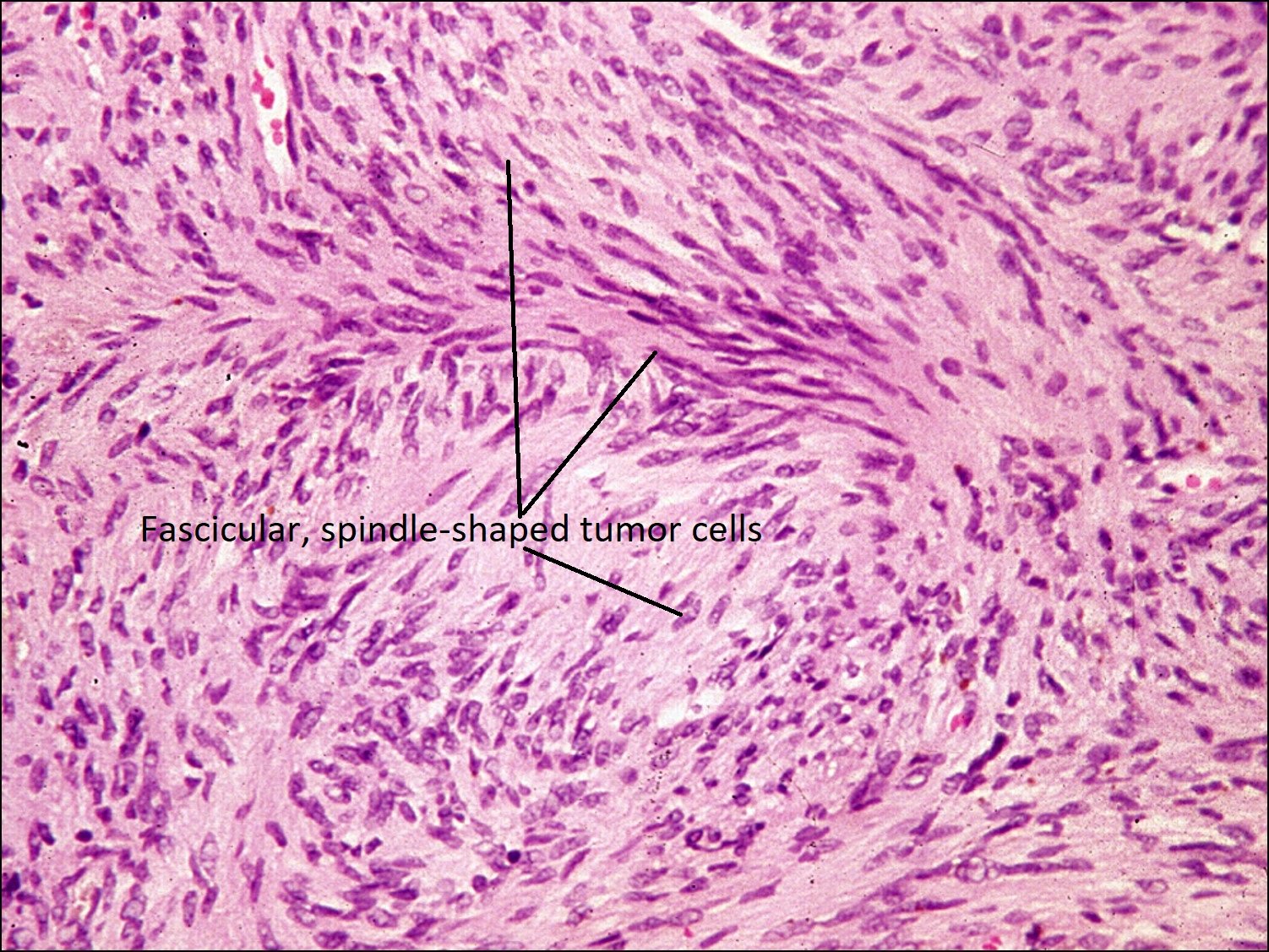
Antoni A type Neurilemmoma


Antoni B type Neurilemmoma
- Intraconal tumor of the optic nerve sheath arising from Schwann cells
- Since optic nerve myelinated by oligodendrocytes, source of Schwann cells likely from sympathetic innervation to the vascular supply of the optic nerve and sheath
- AKA neurilemmoma
- Very uncommon tumor of the optic nerve
- Two histopathologictypes:
- Antoni A: fascicular, spindle-shaped cells
- Antoni B: whitish, myxoid tissue background
- Histopathologic type does not affect prognosis
References:
Harper RA. Basic Ophthalmology. Amer Academy of Ophthalmology; 2010.Yanoff M, Fine BS. Ocular Pathology, A Text and Atlas. Lippincott Williams & Wilkins; 1989.