
Birdshot Chorioretinopathy
Home / Ophthalmic Pathology / Retina and Retinal Pigment Epithelium
Title: Birdshot Chorioretinopathy, Case Report
Author: Taylor Fields, Fourth Year Medical Student, Medical College of Georgia
Photographers: Cyrie Fry, CRA, and Paula Morris, CRA.
Date: 08/23/15
Secondary CORE Category: Retina and Vitreous / Focal and Diffuse Choroidal and Retinal Inflammation
Keywords/Main Subject: Posterior Uveitis; Chorioretinopathy; Birdshot; BSCR; BCR Diagnosis- Birdshot Chorioretinopathy
Brief Description of Case:
This case is a 52-year-old white female who presented complaining of “hundreds of floaters” that had been progressing for several months in both eyes. She noted a crescent shape to the floaters and a one month of a small blurry spot in the inferonasal visual field in her right eye. She also described nyctalopia, a less vivid quality to her vision and morning photopsias and black spots upon awakening that lasted about 30 minutes.
Visual acuity was 20/20 in each eye and intraocular pressure by tonopen was 21 and 19 in the right and left eyes respectively. Her pupillary exam, visual fields, color vision and motility were all normal. The Fundus exam revealed 1+ disc edema, bilateral epiretinal membranes, narrowing of her retinal vessels and numerous mid-peripheral white/yellow choroidal spots bilaterally (Pictures 1-4). ICG photos revealed areas of decreased dye perfusion within the choroid (Picture 3).
The differential diagnosis included inflammatory uveitis (birdshot chorioretinopathy, sarcoidosis), infectious causes (TB, syphilis, Lyme disease) and masquerade syndromes such as choroidal lymphoma. She was found to be HLA-A29 positive. An extensive laboratory work-up was otherwise negative. Full-field electroretinograms (ffERGs) showed attenuated scotopic dim blue flash ERGs to about 59% with slowed photopic b-wave time of 35 milliseconds.
Diagnosis
The patient was diagnosed with birdshot chorioretinopathy (BSCR). Her fundus exam and ffERG results are typical of early stages of BSCR. This disease is an idiopathic posterior uveitis that commonly presents in Caucasians in their sixth decade of life. It has a strong association with the human leukocyte antigen HLA-A29 (96% of patients are carriers).1,2 BSCR typically presents with a gradual centripetal loss of vision and presence of floaters.3
Treatment
The patient was started on a 60 mg prednisone taper as well as mycophenolate and cyclosporine. Systemic immunomodulatory therapy is the mainstay of treatment for BSCR. Concomitant therapy with an antimetabolite and a T-cell inhibitor can be beneficial for preserving vision, and decreasing the cumulative glucocorticoid dose.4,5
Prognosis
BSCR is considered a chronic and progressive isolated ocular disorder. A majority of patients develop retinal dysfunction; however, central vision is typically spared until late in the disease. Visual acuity at initial presentation is a prognostic factor for long-term visual outcomes with appropriate treatment.6
Images

Picture 1. Full color montage photos of the right (A) and left (B) eyes. These show characteristic pisiform lesions of BSCR within the periphery of the retina (black arrows).
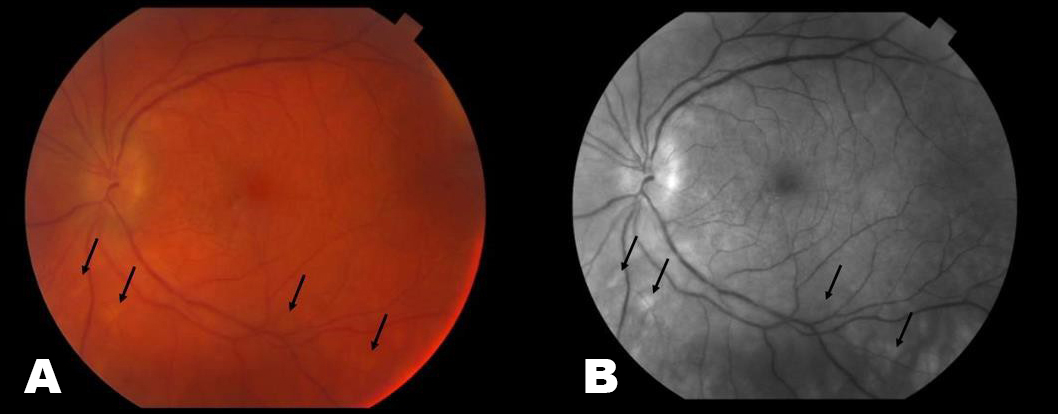
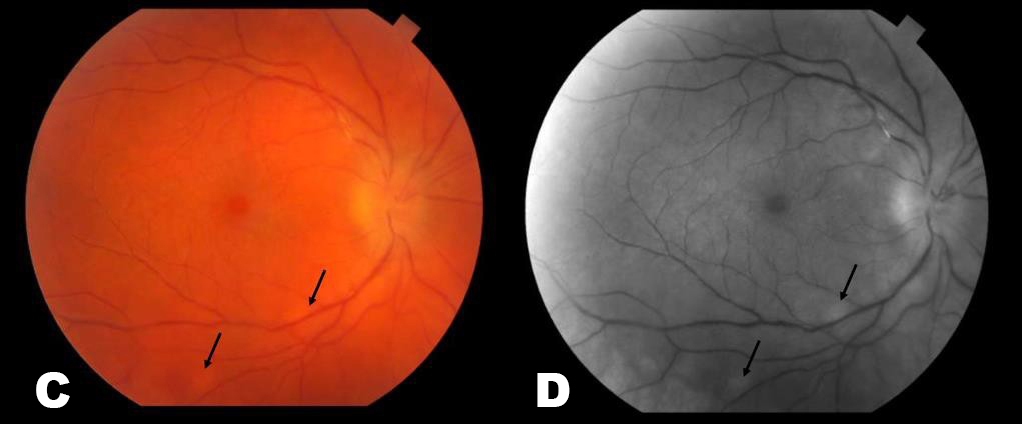
Picture 2. These are color (A & C) and red free (B & D) photos of the left (A & B) and right (C & D) fundi. The periphery has areas of white/yellow choroidal spots (black arrows). There is also narrowing of vessels and disc edema present.
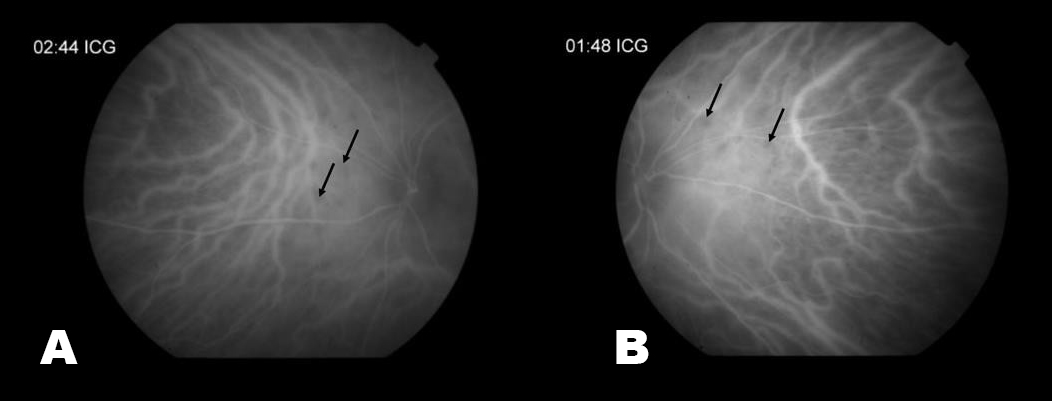
Picture 3. These are late ICG photos of the nasal portions of the Left (A) and Right (B) retinas. There is decreased choroidal perfusion, and thus dark spots, in the areas of inflammation (black arrows).

Picture 4. These are wide field fluorescein angiograms (FA) of the right (A) and left (B) fundi. This shows vasculature leakage, periphlebitis, and disc edema.
Summary of Case
This is a 52 year-old white female diagnosed with birdshot chorioretinopathy who presented with several months of worsening floaters and was found to have the characteristic midperipheral white/yellow choroidal lesions bilaterally. She was found to be HLA-A29 positive, confirmatory of the diagnosis.
References
Levinson RD, Brezin A, Rothova A, et al. Research criteria for the diagnosis of birdshot chorioretinopathy: results of an international consensus Am J Ophthalmol 2006; 141:185 – 187.
- Brézin AP, Monnet D, Cohen JH, Levinson HLA-A29 and birdshot chorioretinopathy.Ocul Immunol Inflamm. 2011;19(6):397-400.
- Shah KH, Levinson RD, Yu F, et al. Birdshot chorioretinopathy. Surv Ophthalmol 2005; 50:519 –
- Becker MD, Wertheim MS, Smith JR, Rosenbaum Long-term follow-up of patients with birdshot retinochoroidopathy treated with systemic immunosuppression. Ocul Immunol Inflamm 2005; 13:289–293.st
- Kiss, Szilard, Ahmed, Muna, Letko, Erik, & Foster, Stephen. (2005). Long-term Follow- up of Patients with Birdshot Retinochoroidopathy Treated with Corticosteroid-Sparing Systemic Immunomodulatory Therapy. Ophthalmology, 112(6), 1066-1071.e2.
- Tomkins-Netzer O, Taylor SR, Lightman Long-term clinical and anatomic outcome of birdshot chorioretinopathy. JAMA Ophthalmol 2014; 132:57 – 62.
Faculty Approval by: Griffin Jardine, MD
Identifier: Moran_CORE_23873
Opthalmoplegic Migraine/Recurrent Painful Ophthalmoplegic Neuropathy
Home / Neuro-Ophthalmology / Evaluation of Diplopia
Title: Opthalmoplegic Migraine/Recurrent Painful Ophthalmoplegic Neuropathy
Author Information: Ryan O’Meilia MS4, University of Oklahoma; Judith Warner MD, John A. Moran Eye Center
Financial Disclosure: None
Date: September 2015
Keywords: Opthalmoplegic Migraine; Recurrent Painful Ophthalmoplegic neuropathy
Description:
Chief Complaint: Lid drooping and drifting eye
History of Present Illness:
This case discusses a 3 year old girl with a symptomatic, recurring oculomotor palsy. Her first episode was at age one but completely resolved. Four days prior to her most recent presentation she had a gastroenteritis with vomiting and decreased energy. Her parents did not note a fever, upper respiratory infection, cough, eye pain, rash or HA in the past few weeks. The gastroenteritis resolved two days later but around that same time she developed right ptosis. Over the next two days the eyelid drooping progressed and the patient developed deviated eye and asymmetric pupils.
Her previous episode of oculomotor nerve palsy developed much like the present one. The parents report a sub-acute onset over a few days that progressed from ptosis, to anisocoria and strabismus. The episode resolved without treatment over about one week. An MRI was performed at an outside hospital and the read was as follows: “Enhancement of the right third cranial nerve (CN) which is most prominent immediately adjacent to the origin of the nerve at the brain stem. The enhancement extends anteriorly along the nerve to the cavernous sinus.” Her clinical presentation and imaging were felt to be consistent with inflammatory neuritis, most likely post viral.
Past Medical History: otherwise non-contributory
Past Surgical History: None
Medications: None
Allergies: No known drug allergies
Immunizations: Up to date
Development: Age appropriate
Family History: No family history of eye disease, migraine, MS, neurologic disease, childhood cancers. Maternal cousins with celiac disease and DM1
Social History: Lives with parents; 2 cats and a dog. Attends daycare
Review of Symptoms: All negative except as above
Ocular Physical Exam:
- General: Alert and oriented, NAD
- Visual Acuity: Fix and Follow OU
- Pupils
- OD: 5mm > 4mm
- OS: 4mm > 2mm
- EOM
- Primary gaze: right eye deviated inferiorly and temporally
- OD:
- -3 adduction
- -2 elevation
- -1 depression
- -0 abduction
- OS:
- Penlight
- Full EOM
- Orbits: No deformities, ecchymosis or edema
- Lids/Lashes: Right ptosis, MRD1 5mm, normal eyelid position OS
- Conjunctiva/Sclera: white and quiet OU
- Cornea: clear OU
- Anterior Chamber: formed without hyphema or hypopyon OU
- Iris: flat and round OU
- Lens: WNL OU
- Dilated Fundus exam:
- Optic Nerve: sharp margins, no disc edema
- Macula: Healthy OU
- Vessels: Normal caliber OU
- Periphery: WNL OU
Vital signs and labs:
T: 36.8
HR: 104
RR: 24
BP: 112/60
- Sat: 99% RA
- CRP, BMP CBC: within normal limits
Imaging:

Image 1: Axial MRI T1 with contrast showing enhancement of the right 3rd nerve in the cisternal segment.

Image 2: Coronal MRI T1 with contrast showing enhancement and thickening of the cisternal portion of the right oculomotor nerve.
Differential:
- Post-Viral Neuritis
- Ophthalmoplegic migraine/Recurrent painful ophthalmoplegic neuropathy (OM/RPON)
- Aneurysm
- Schwannoma
- Tolosa-Hunt
- ADEM
- Miller-Fisher Syndrome
- TB, Lyme, Sarcoid, Lymphoma
Case Discussion:
Based on clinical presentation, the list of differential diagnoses for our patient’s third nerve palsy would be quite extensive. ADEM and Miller-Fischer syndrome can present as third nerve palsies but they would also tend to be accompanied by other neurologic deficits such as ataxia or areflexia. When the recurrent and resolving history is taken into account aneurysm, schwannoma, TB, Lyme, sarcoid, and lymphoma become less likely as these would tend to be slowly progressive and unlikely to resolve without treatment. Imaging confirms the absence of schwannoma and also rules out Tolosa-hunt which would show inflammation in the cavernous sinus and meningeal enhancement. Aneurysm, Tolosa-Hunt, and Miller-Fisher syndrome would also be quite rare in this age group.
With all of these factors taken together the most likely diagnosis is either post-viral neuritis or Ophthalmoplegic migraine/Recurrent painful ophthalmoplegic neuropathy (OM/RPON). It is possible that these two conditions are related.
Epidemiology
OM/RPON is a rare condition with a prevalence of 0.7 per million6; it usually begins in childhood.2,3 A systematic review authored by Gelfand found a median age of onset at 8 years old (interquartile range 3, 16). They also found that approximately 2/3 of patients affected by OM/RPON were female. 4
Signs and Symptoms
OM/RPON typically presents as a headache followed by ophthalmoplegia. If aheadache is present, it is typically unilateral and ipsilateral to the affected eye. The headache may or may not have migrainous features: photophobia, phonophobia, or nausea/vomiting. The ophthalmoplegia can occur immediately or up to 14 days after the headache. One or multiple nerves may be also be involved. The frequency of nerves affected in Gelfand’s paper was CN III 83%, CNVI 20%, and CNIV 2%. If multiple nerves were affected, CNIII was always included.4 When CNIII is affected it may be a partial or complete palsy. Both ptosis and mydriasis are common, especially among children.
Diagnostic Criteria
The diagnostic criteria have according to the International Classification of Headache Disorder 3-beta1 are:
- At least two attacks fulfilling criterion
- Unilateral headache accompanied by ipsilateral paresis of one, two or all three ocular motor
- Orbital, parasellar, or posterior fossa lesion has been excluded by appropriate
- Not better accounted for by another ICHD-3 diagnosis
As stated above, before the diagnosis of OM/RPON is made it is critically important to rule out other possible etiologies such as aneurysm, schwannoma, granulomatous disease, and inflammatory neuropathy.2
Pathophysiology
The pathophysiology of OM/RPON is a topic of ongoing debate. The diagnostic criteria in ICHD have been updated over the years to mirror the trends in the etiologic discussion by classifying it first as a migraine, then as a neuralgia, and most recently as a neuropathy.5 In fact, with the newest release of ICHD-3beta, the International Headache Society recommended the term ‘ophthalmoplegic migraine’ be abandoned.1 The driving force for this progression has been the need to explain the reversible contrast enhancement at the root entry zone of the affected cranial nerve.
Some who support the viewpoint of a neuropathy will point to the possibility of a benign neurotropic viral infection and highlight the similarities of the imaging in OM/RPON to those found in Bell’s Palsy.2 Others advocate for an immune-mediated neuropathy similar to chronic inflammatory demyelinating polyneuropathy (CIDP).5 In both of these explanations, the headache of OM/RPON is a result of inflammation of the nerve. The inflammation causes vasoconstriction of the nearby vasculature subsequently triggering the headache. However, these hypotheses are not without their weaknesses, CSF analysis and viral studies typically return unremarkable in OM/RPON.
Even with the current trend towards viewing OM/RPON as a neuropathy, there are still some who continue to advocate for a migrainous etiology. A paper published in 2014 proposed that a migraine induced vasospasm of the arteries supplying CNIII, IV, or VI could lead to ischemia of the nerves causing reversible breakdown of the nerve-blood barrier allowing for contrast extravasation and subsequent nerve enhancement on MRI.3 The authors make a great case, yet still leave questions unanswered. If migraine is the causal process then why does treatment with acute and prophylactic migraine medication offer little to no benefit or protection to patients?
In summary, there is still much work to be done towards reaching an understanding of how and why OM/RPON occurs. It is valuable to consider that OM/RPON may in fact have a multifactorial etiology resulting from processes and predispositions related to both neuropathy and migraine.
Treatment
With such ambiguity clouding the pathophysiology of OM/RPON it follows that there is also uncertainty regarding effective treatment for the condition.
Migraine medications both acute and prophylactic have been tried with unconvincing efficacy while the results of steroids have been positive yet mixed. Gelfand found steroids to be beneficial in 54% of cases reviewed. Yet the effects were either unclear, not beneficial or even harmful in 35%, 8%, and 4% respectively.4
Prognosis
Prognosis in OM/RPON is generally excellent and most patients can experience a full recovery in days to weeks. However small minority of patients may be left with persistent neurological deficits, especially those who suffer from repeated attacks.2,3,4,5
Faculty Approval by: Griffin Jardine, MD
Identifier: Moran_CORE_23858
References
- The International Classification of Headache Disorders, 3rd edition (beta version).
- Alexander, Al. Ophthalmoplegic Migraine: Reversible Enhancement and Thickening of the Cisternal Segment of the Oculomotor Nerve on Contrast-Enhanced MR Images. AJNR Am J Neuroradiol 19:1887–1891, November 1998
- Ambrosetto, Al. Ophthalmoplegic migraine: From questions to answers. Cephalalgia 2014, Vol. 34(11) 914–919
- Gelfand, Al. Ophthalmoplegic ‘‘Migraine’’ or Recurrent Ophthalmoplegic Cranial Neuropathy: New Cases and a Systematic Review. Journal of Child Neurology 27(6) 759-766. 2012
- Fö rderreuther, From Ophthalmoplegic Migraine to Cranial Neuropathy. Curr Pain Headache Rep (2015) 19: 21 DOI 10.1007/s11916-015-0492-1
- Quisling, Ophthalmoplegic Migraine: 30-year-old male with migraine headaches and occasional diplopia. http://webeye.ophth.uiowa.edu/eyeforum/cases/52-Ophthalmoplegic- Migraine-Diplopia-Headache.htm
Parry-Romberg Syndrome
Home / Orbit, Eyelids, and Lacrimal System / Periocular Malpositions and Involutional Changes
Title: Parry-Romberg Syndrome Case Report
Author: Rebekah Gensure, PhD, 4th Year Medical Student, Rutgers Robert Wood Johnson Medical School; Laura Hanson, MD, Neuro-Ophthalmology Fellow, John A. Moran Eye Center; Kathleen Digre, MD, John A. Moran Eye Center
Photographer: James Gilman
Date: July 20, 2015
Moran CORE: Orbits, Eyelids, and Lacrimal System/Periocular Malpositions and Involutional Changes/Involutional Periorbital Changes
Keywords/Main Subjects: Parry-Romberg Syndrome, hemifacial atrophy
Diagnosis/Differential Diagnosis: Parry-Romberg Syndrome, post traumatic fat atrophy, hemifacial microsomia (first and second branchial arch syndrome), Goldenhar’s syndrome
Brief Description of Case:
HPI:
A 27-year-old female patient presented with a long history of facial asymmetry and right tongue atrophy. She was diagnosed with Parry-Romberg syndrome 7 years ago, at the age of 20. At the time of her initial diagnosis at an outside institution, the patient report experiencing significant facial pain and wasted facial appearance that had been present for many years and had gone undiagnosed until that point. Presently, the patient is status-post surgical repair (hemifacial fat grafting) with a satisfactory cosmetic result.
The patient also has a history of migraine headache. At the time of the most recent visit, the patient reported improvement in migraine headaches with no preventative medications currently. Headaches have been less frequent (approximately 1 every 2 weeks) and pain rating no worse than 5/10. She also reports episodic ptosis, which appears to be related to migraine and menstrual cycle.
Other ocular history includes a history of treated amblyopia secondary to accommodative esotropia and is still in spectacle correction.
Exam: OCULAR:
Best corrected visual acuities: 20/20 OD and 20/20 OS.
Pupils: 3mm OU light, 7 mm OU dark; briskly reactive OU with no RAPD EOM: -½ OD on right gaze; Orthotropic at distance; exophoria at near Exophthalmometry: 13 mm OD, 16 mm OS
Color Vision: 10/10 OU Ishihara
Stereo Vision: +Fly, 3/3 animals, 7/9 circles IOP: 16 mm Hg OD & OS.
VF: Full OU
SLE: Anterior segment within normal limits
Fundus: Within normal limits; C/D ratio 0.1 OD, 0.2 OS Refraction: OD +2.50 sphere, +0.75 cylinder at axis 25
OS +1.50 sphere, +1.50 cylinder at axis 130
NEURO: Completely normal neurological examination except for the facial asymmetry.
Discussion:
Hemifacial atrophy, also known as Parry-Romberg syndrome, is characterized by a slow progressive deterioration (atrophy) of the skin and subcutaneous tissue structures on half of the face [1]. As it is described by Parry, Henoch and Romberg in the early 19th century, there is wasting of the subcutaneous fat with or without atrophy of adjacent skin, bone, and cartilage [2- 3]. The condition is typically insidious in onset, and progression is variable. In some cases, atrophy may halt before the entire hemi-face is involved but with residual disability [4]. In mild cases, there may be only minor cosmetic effects without any disability.
Because of the relative rarity of this condition, associated clinical conditions have mostly been identified through case reports. For example, in 1985, Sagild and Alving reported a case associating hemiplegic migraine with hemifacial atrophy [5]. Seizures are also commonly reported to co-occur with hemifacial atrophy, particularly contralateral simple partial or generalized seizures [6]. Additionally, Parry-Romberg syndrome has sometimes been associated with localized scleroderma, although this association remains controversial.
Long-term progression of the condition has not been well documented; however, one interesting case report followed several patients over time, including one patient who was followed for over 43 years [7]. For this particular long-term follow-up patient, progression of facial atrophy appeared to progress until age 15 but then slow or stop until age 23, at which point new onset hyperreflexia of the contralateral lower extremity was noted. Over the years, the facial atrophy remained apparently stable, although his neurological function gradually declined; by age 58, he demonstrated wide-based gait with absent plantar and tendon reflexes, mildly diminished pain and temperature sensation, end-position nystagmus, and difficulty with heel-to-shin and tandem testing.
Treatment options are limited for patients diagnosed with Parry-Romberg hemifacial atrophy. Currently, there are no known therapies that will stop progression of the disease.
Reconstruction has been utilized, with variable results depending on the timing of the intervention. For the best results possible, timing of surgery should be strategized according to when the disease appears to have exhausted its course and facial growth is completed [4].
Images or Video:
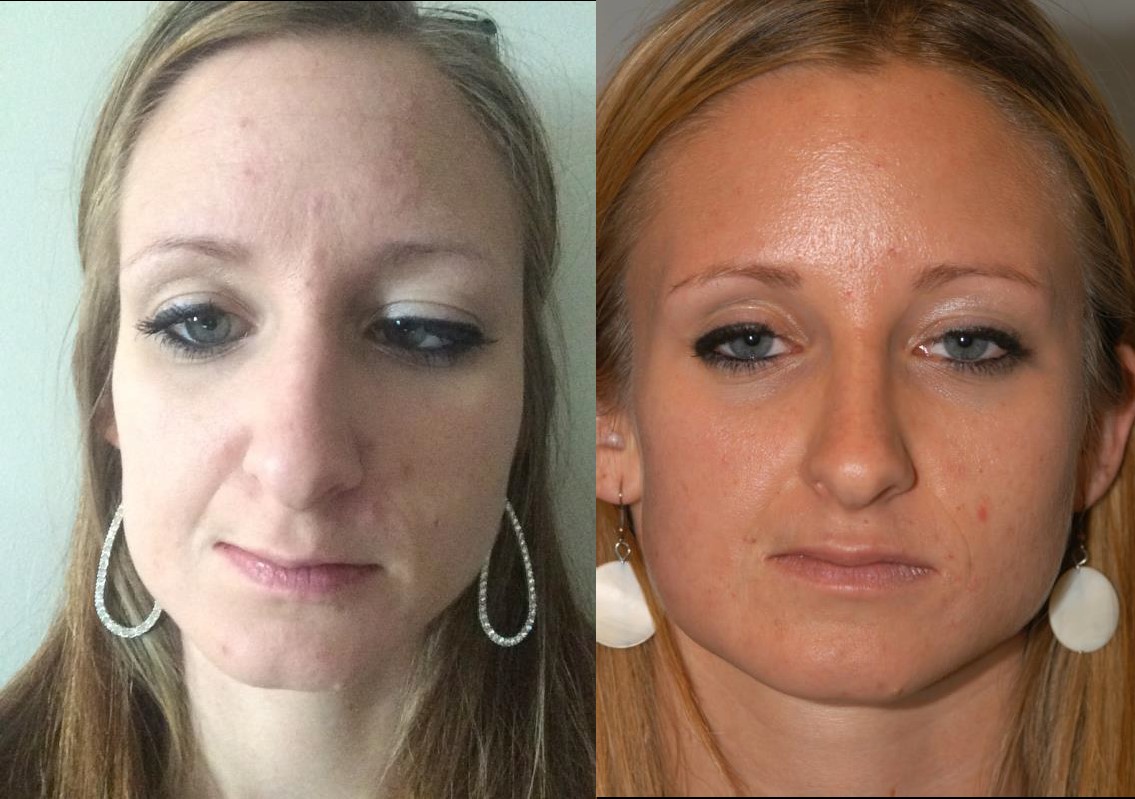
Figure 1 a): Right hemifacial atrophy at baseline in patient previously diagnosed with Parry- Romberg syndrome; b): Patient with Parry-Romberg syndrome with history of right hemifacial atrophy, status post fat grafting, with satisfactory cosmetic result. (Photographs courtesy of the patient)

Figure 2: Tongue hemiatrophy in patient with diagnosed Parry-Romberg syndrome. (Photograph by James Gilman)

Figure 3: Right enophthalmos observed in patient with Parry-Romberg syndrome with right hemifacial atrophy. Hertel measurements indicated posterior displacement of 3 mm on the affected side (right) compared to the unaffected (left) side. (Photographs by James Gilman)
Summary of the Case:
The patient is a 27-year-old woman with Parry-Romberg syndrome with hemifacial atrophy, status-post reconstructive surgical repair with a satisfactory cosmetic result. Overall, the patient is quite stable, with no major new changes in facial structure visible on external exam as compared to prior exams. Based on the apparent stability of the disease process and satisfaction of the patient with her appearance, the patient was recommended to return to clinic only for yearly follow-up or sooner as needed.
References:
- Esan T and Olusile Hemifacial Atrophy: A Case Report And Review Of Literature. The Internet Journal of Dental Science. 2003. 1(1).
- Parry Collections from the unpublished medical writings of the late Caleb Hillier Parry, M.D., F.R.S. 1825 London: Underwoods. 478–80.
- Romberg, MH; Henoch, EH (1846). Krankheiten des nervensystems (IV: Trophoneurosen). Klinische ergebnisse (in German). Berlin: Albert Förstner. 75–81.
- NINDS Parry-Romberg Information Page [Internet]. Bethesda: Office of Communications and Public Liaison, National Institute of Neurological Disorders and Stroke, National Institutes of Health; January 25, Available from: http://www.ninds.nih.gov/disorders/parry_romberg/parry_romberg.htm
- Sagild JC and Alving Hemiplegic migraine and progressive hemifacial atrophy; June 1985; 17(6): 620.
- Wolf SM and Verity Neurological complications of progressive facial hemiatrophy. J Neurol Neurosurg Psychiatry. 1974 Sep; 37(9): 997–1004.
- Asher SW and Berg Progressive hemifacial atrophy: Report of three cases, including one observed over 43 years, and computed tomography findings. Arch Neurol. 1982; 39: 44-46.
Faculty Reviewer: Griffin Jardine, MD
Copyright statement: Copyright 2017. Please see terms of use page for more information.
Band Keratopathy
Home / External Disease and Cornea / Clinical Approach to Depositions and Degenerations of the Conjunctiva, Cornea, and Sclera
Title: Band Keratopathy Case Report
Author: Martin de la Presa, BA
Photographer: unknown
Date: 8/18/2015

Keywords / Main Subjects: Band keratopathy; calcium hydroxyapatite deposition
Diagnosis / Differential Diagnosis: Interstitial keratitis; calcareous degeneration; calciphylaxis
Secondary CORE Category: Intraocular Inflammation and Uveitis / Complications of Uveitis
Brief Description of Image: Band keratopathy is the pathological deposition of calcium within the superficial layers of the cornea, specifically Bowman’s layer. The condition ranges from asymptomatic to causing ocular irritation, foreign body sensation and decreased vision. Though it is often idiopathic there is a broad differential of local and systemic associated diseases. The local causes include chronic ocular irritation or inflammatory conditions such as chronic anterior uveitis (especially in Juvenile Idiopathic Arthritis), interstitial keratitis, superficial keratitis, phthisis bulbi, end-stage glaucoma and silicone oil left in the aphakic eye. Systemic diseases associations include those diseases that elevate serum calcium levels such as in hyperparathyroidism, sarcoidosis, multiple myeloma, hypophosphatemia, Paget disease and chronic renal failure.
On exam, there is a white band-like formation of calcium across the corneal surface with irregular boarders and a peripheral clearing of cornea between the calcium deposits and the limbus. The calcium deposition is typically found beneath the epithelial layer within Bowman’s layer but may extend into anterior stroma. In the absence of an explainable local etiology laboratory testing is recommended to assess serum calcium and phosphate levels and renal function. When symptomatic, the calcium deposits can be removed with superficial debridement and manual scraping of the corneal surface with or without the aid of a chelating agent such as ethylenediaminetetraacetic acid (EDTA). Recurrence is common unless the predisposing cause is identified and treated.
Faculty Approval: Griffin Jardine, MD
Identifier: Moran_CORE_23763
References:
Copyright statement: Copyright 2017. Please see terms of use page for more information.
A Case Report of Hypertensive Retinopathy
Home / Retina and Vitreous / Other Retinal Vascular Diseases
Title: A Case Report of Hypertensive Retinopathy
Author: Tyler Scott Quist, BS
Photographer: James Gilman
Date: 08/2016
Keywords/Main Subjects: Hypertensive retinopathy, hypertensive emergency
Introduction:
Hypertensive retinopathy refers to the microvascular changes of the retina that occur in the setting of hypertension and is a common cause of ocular disease. Hypertensive emergency refers to a systolic blood pressure (SBP) ≥ 180 and/or diastolic blood pressure (DBP) ≥ 120 with evidence of end organ damage, such as retinopathy.
Case Report:
A 40-year-old male with a history of newly diagnosed systolic blood pressure over 200 presents with a three-week history of bilateral blurry vision and halos worse in the left eye. The patient reported new-onset migraines and denied any other ocular symptoms. On exam, his visual acuity was 20/25 and 20/150 in the right and left eye, respectively. Tonometry, pupils, visual fields, extraocular movements, and slit lamp exam were unremarkable. The fundus exam was remarkable for bilateral optic disc edema and hemorrhage, macular hemorrhages and exudates, and arteriolar narrowing as shown in Figure 1. The patient was sent to the emergency department, where magnetic resonance imaging (MRI) revealed a small stroke in the corpus collosum. The patient was treated for hypertensive emergency with antihypertensives and his vision slowly improved over the course of several months.

Figure 1: Hypertensive retinopathy in the right eye remarkable for bilateral optic disc edema and hemorrhage, macular exudates and hemorrhages, as well as arteriolar narrowing.
Discussion:
Hypertension results in retinal microvascular changes called hypertensive retinopathy, which may be categorized as mild, moderate, or severe. The mild form is characterized by retinal arteriolar narrowing, the moderate form is characterized by hemorrhages and exudates, and the severe form is characterized by optic disc edema1. Hypertensive retinopathy is more common with increased age and among black persons and has a prevalence rate from two to fifteen percent1. Patients with malignant hypertensive retinopathy may present with blurry vision, decreased visual acuity, eye pain, and headaches. The dilated fundoscopic exam and coexisting hypertension is paramount in establishing the correct diagnosis and classification of the disease. Previously published literature has shown that reducing systemic blood pressure below 140/90 mmHg improves hypertensive retinopathy2,3. However, it is uncertain whether antihypertensive agents with a direct effect on microvasculature have any benefit over other antihypertensive medications.
References:
- Wong TY, Mitchell P. Hypertensive retinopathy. N Engl J Med 2004;351:2310.
- Bock KD. Regression of retinal vascular changes by antihypertensive therapy. Hypertension 1984;6:III-158.
- Dahlof B, Stenkula S, Hansson L. Hypertensive retinal vascular changes: relationship to left ventricular hypertrophy and arteriolar changes before and after treatment. Blood Press 1992;1:35-44.
Faculty Approval By: Dr. Amy Lin
Footer: Copyright 2016, Tyler Scott Quist. For further information regarding the rights to this collection, please visit: http://morancore.utah.edu/terms-of-use/
Identifier: Moran_CORE_21698
Disclosure (Financial or other): No authors have any financial or proprietary interest in any material or methods mentioned.
UNDER REVIEW
Opthalmoplegic Migraine / Recurrent Painful Ophthalmoplegic Neuropathy
Home / Pediatric Ophthalmology and Strabismus / Special Forms of Strabismus
Title: Opthalmoplegic Migraine / Recurrent Painful Ophthalmoplegic neuropathy
Date: 09/2015
Keywords: Opthalmoplegic Migraine, Recurrent Painful Ophthalmoplegic neuropathy
Images:

Brain MRI T-1 with contrast axial cut

Brian MRI T-1 with contrast coronal cut
Case Report:
Chief Complaint: Lid drooping and drifting eye
History of Present Illness: 3 year 3month old girl with past medical history of oculomotor nerve palsy (episode 2 years prior, resolved) presents with recurrent symptoms of oculomotor palsy. Four days prior, she experienced a GI illness with vomiting and decreased energy. Her parents deny fever, upper respiratory infection, cough, eye pain, rash or HA. The GI illness resolved two days later and around the same time her right upper eyelid began to droop. Over the next two days the drooping progressed and the patient developed deviated eye and asymmetric pupils. Her previous episode of oculomotor nerve palsy developed much like the present one. The parents report a sub-acute onset over a few days that progressed from ptosis, to anisocoria and strabismus. The episode resolved without treatment over about one week. An MRI was performed at an outside hospital and the read was as follows: “Enhancement of the right third cranial nerve which is most prominent immediately adjacent to the origin of the nerve at the brain stem. The enhancement extends anteriorly along the nerve to the cavernous sinus.” Her clinical presentation and imaging were felt to be consistent with inflammatory neuritis, most likely post viral.
Past Medical History: Otherwise non-contributory
Past Surgical History: None
Medications: None
Allergies: No known drug allergies
Immunizations: Up to date
Development: Age appropriate
Family History: No family history of eye disease, migraine, MS, neurologic disease, childhood cancers. Maternal cousins with celiac disease and DM1
Social History: Lives with parents; 2 cats and a dog. Attends daycare
Review of Symptoms: All negative except as above
Ocular Physical Exam:
- General: Alert and oriented, NAD
- isual Acuity: Fix and Follow OU
- Pupils
- OD: 5mm > 4mm
- OS: 4mm > 2mm
- EOM
- Primary gaze: right eye deviated inferiorly and temporally
- OD:
- -3 adduction
- -2 elevation
- -1 depression
- -0 abduction
- OS:
- Full EOM
- Penlight
- Orbits: No deformities, ecchymosis or edema
- Lids/Lashes: Right ptosis, MRD1 0.5mm, normal eyelid position OS
- Conjunctiva/Sclera: white and quiet OU
- Cornea: clear OU
- Anterior Chamber: formed without hyphema or hypopyon OU
- Iris: flat and round OU
- Lens: WNL OU
- Dilated Fundus exam:
- Optic Nerve: sharp margins, no disc edema
- Macula: Healthy OU
- Vessels: Normal caliber OU
- Periphery: WNL OU
Vital signs and labs:
- T: 36.8
- HR: 104
- RR: 24
- BP: 112/60
- Sat: 99% RA
- CRP, BMP CBC: within normal limits
Imaging:
Image 1: Axial MRI T1 with contrast showing enhancement of the right 3rd nerve in the cisternal segment.
Image 2: Coronal MRI T1 with contrast showing enhancement and thickening of the cisternal portion of the right oculomotor nerve.
Differential:
- Post-Viral Neuritis
- Ophthalmoplegic migraine/Recurrent painful ophthalmoplegic neuropathy
- Aneurysm
- Schwannoma
- Tolosa-Hunt
- ADEM
- Miller-Fisher Syndrome
- TB, Lyme, Sarcoid, Lymphoma
Case Discussion:
Based on clinical presentation, the list of differential diagnoses for our patient’s third nerve palsy would be quite extensive. ADEM and Miller-Fischer syndrome can present as third nerve palsies but they would also tend to be accompanied by other neurologic deficits such as ataxia or areflexia. When the recurrent and resolving history is taken into account aneurysm, schwannoma, TB, Lyme, sarcoid, and lymphoma become less likely as these would tend to be slowly progressive and unlikely to resolve without treatment. Imaging confirms the absence of schwannoma and also rules out Tolosa-hunt which would show inflammation in the cavernous sinus and meningeal enhancement. Aneurysm, Tolosa-Hunt, and Miller-Fisher syndrome would also be quite rare in this age group.
With all of these factors taken together the most likely diagnosis is either post-viral neuritis or Ophthalmoplegic migraine/Recurrent painful ophthalmoplegic neuropathy (OM/RPON). It is possible that these two conditions are related.
Epidemiology
OM/RPON is a rare condition with a prevalence of 0.7 per million6; it usually begins in childhood.2,3 A systematic review authored by Gelfand found a median age of onset at 8 years old (interquartile range 3, 16). They also found that approximately 2/3 of patients affected by OM/RPON were female. 4
Signs and Symptoms
OM/RPON typically presents as a headache followed ophthalmoplegia. If headache is present, it is typically unilateral and ipsilateral to the affected eye. The headache may or may not have migrainous features; accompanied by photophobia, phonophobia, or nausea/vomiting. The ophthalmoplegia can occur immediately or up to 14 days after the headache. One or multiple nerves may be affected. The frequency of nerves affected in Gelfand’s paper was CNIII 83%, CNVI 20%, and CNIV 2%. If multiple nerves were affected, CNIII was always included.4 When CNIII is affected it may be a partial or complete palsy. Both ptosis and mydriasis are common, especially among children.
Diagnostic Criteria:
According to the International Classification of Headache Disorder 3-beta1:
A. At least Two attacks fulfilling criterion B.
B. Unilateral headache accompanied by ipsilateral paresis of one, two or all three ocular motor nerves.
C. Orbital, parasellar, or posterior fossa lesion has been excluded by appropriate investigation.
D. Not better accounted for by another ICHD-3 dx
As stated above, before the diagnosis of OM/RPON is made it is very important to rule out other possible etiologies such as aneurysm, schwannoma, granulomatous disease, and inflammatory neuropathy.2
Pathophysiology:
The pathophysiology of OM/RPON is a topic of ongoing debate. The diagnostic criteria in ICHD have been updated over the years to mirror the trends in the etiologic discussion by classifying it first as a migraine, then as a neuralgia, and most recently as a neuropathy.5 In fact, with the newest release of ICHD-3beta, the International Headache Society recommended the term ‘ophthalmoplegic migraine’ be abandoned.1 The driving force for this progression has been the need to explain the reversible contrast enhancement at the root entry zone of the affected cranial nerve.
Some who support the viewpoint of a neuropathy will point to the possibility of a benign neurotropic viral infection and highlight the similarities of the imaging in OM/RPON to those found in Bell’s Palsy.2 Others advocate for an immune-mediated neuropathy similar to chronic inflammatory demyelinating polyneuropathy (CIDP).5 In both of these explanations, the headache of OM/RPON is a result of inflammation of the nerve. The inflammation causes vasoconstriction of the nearby vasculature subsequently triggering the headache. However, these hypotheses are not without their weaknesses, CSF analysis and viral studies typically return unremarkable in OM/RPON.
Even with the current trend towards viewing OM/RPON as a neuropathy, there are still some who continue to advocate for a migrainous etiology. A paper published in 2014 proposed that a migraine induced vasospasm of the arteries supplying CNIII, IV, or VI could lead to ischemia of the nerves causing reversible breakdown of the nerve-blood barrier allowing for contrast extravasation and subsequent nerve enhancement on MRI.3 The authors make a great case, yet still leave questions unanswered. If migraine is the causal process then why does treatment with acute and prophylactic migraine medication offer little to no benefit or protection to patients?
In summary, there is still much work to be done towards reaching an understanding of how and why OM/RPON occurs. It is valuable to consider that OM/RPON may in fact have a multifactorial etiology resulting from processes and predispositions related to both neuropathy and migraine.
Treatment: With such ambiguity clouding the pathophysiology of OM/RPON it follows that there is also uncertainty regarding effective treatment for the condition. Migraine medications both acute and prophylactic have been tried with unconvincing efficacy while the results of steroids have been positive yet mixed. Gelfand found steroids to be beneficial in 54% of cases reviewed. Yet the effects were either unclear, not beneficial or even harmful in 35%, 8%, and 4% respectively.4
Prognosis: Prognosis in OM/RPON is generally excellent and most patients can experience a full recovery in days to weeks. However small minority of patients may be left with
persistent neurological deficits, especially those who suffer from repeated attacks.2,3,4,5
References
1. The International Classification of Headache Disorders, 3rd edition (beta version).
2. Alexander, et. Al. Ophthalmoplegic Migraine: Reversible Enhancement and Thickening of the Cisternal Segment of the Oculomotor Nerve on Contrast-Enhanced MR Images. AJNR Am J Neuroradiol 19:1887–1891, November 1998
3. Ambrosetto, et. Al. Ophthalmoplegic migraine: From questions to answers. Cephalalgia 2014, Vol. 34(11) 914–919
4. Gelfand, et. Al. Ophthalmoplegic ‘‘Migraine’’ or Recurrent Ophthalmoplegic Cranial Neuropathy: New Cases and a Systematic Review.
Identifier: Moran_CORE_21686
Financial Disclosure: None
Sickle Cell Retinopathy
Home / Retina and Vitreous / Other Retinal Vascular Diseases
Title: Sickle Cell Retinopathy
Author: Elizabeth Ann Urias, MSIV
Photographer:
Date: 06/24/2016
Image or video:

Keywords/Main Subjects: Sickle cell disease; sickle cell retinopathy; microvascular occlusion; retinal hemorrhage; salmon patch;
Diagnosis: Sickle Cell Retinopathy: Salmon Patch Hemorrhage
Description of Image: In sickle cell hemaglobinopathy, RBC sickling causes peripheral retinal arteriolar occlusion, leading to ischemic necrosis and weakening of the vessel walls. Fragile vessels result in hemorrhages in one or more layers of the retina. An intra-retinal hemorrhage is round or oval shaped, bright red, and measures ¼-1 disc diameter. In days or weeks, this bright red color becomes a salmon color, which is known as a “salmon patch.” After time, hemoglobin degradation occurs and the defect appears as bright yellow dots at several layers of the sensory retina, also known as “iridescent bodies.” (Bonanomi & Lavezzo, 2013)
References:
- Bonanomi, M. T. B. C., & Lavezzo, M. M. (2013). Sickle cell retinopathy: diagnosis and treatment. Arquivos Brasileiros de Oftalmologia, 76(5), 320–327.
Faculty Approval by: Griffin Jardine, MD
Identifier: Moran_CORE_21668
Financial Disclosures: None
Copyright statement: Copyright 2017. Please see terms of use page for more information.
Corneal Allograft Rejection Three Years Status Post Penetrating Keratoplasty
Home / External Disease and Cornea / Diagnosis and Management of Immune-Related Disorders of the External Eye
Title: Corneal Allograft Rejection Three Years Status Post Penetrating Keratoplasty
Author: Charlotte L. Marous, B.S., M.S.G.H.; Brian E. Zaugg M.D. July 2016
Photographer: James Gilman
Image or Video:

Figure 1: Slit lamp photo demonstrating healthy corneal graft with full clarity and intact sutures status post penetrating keratoplasty for keratoconus.
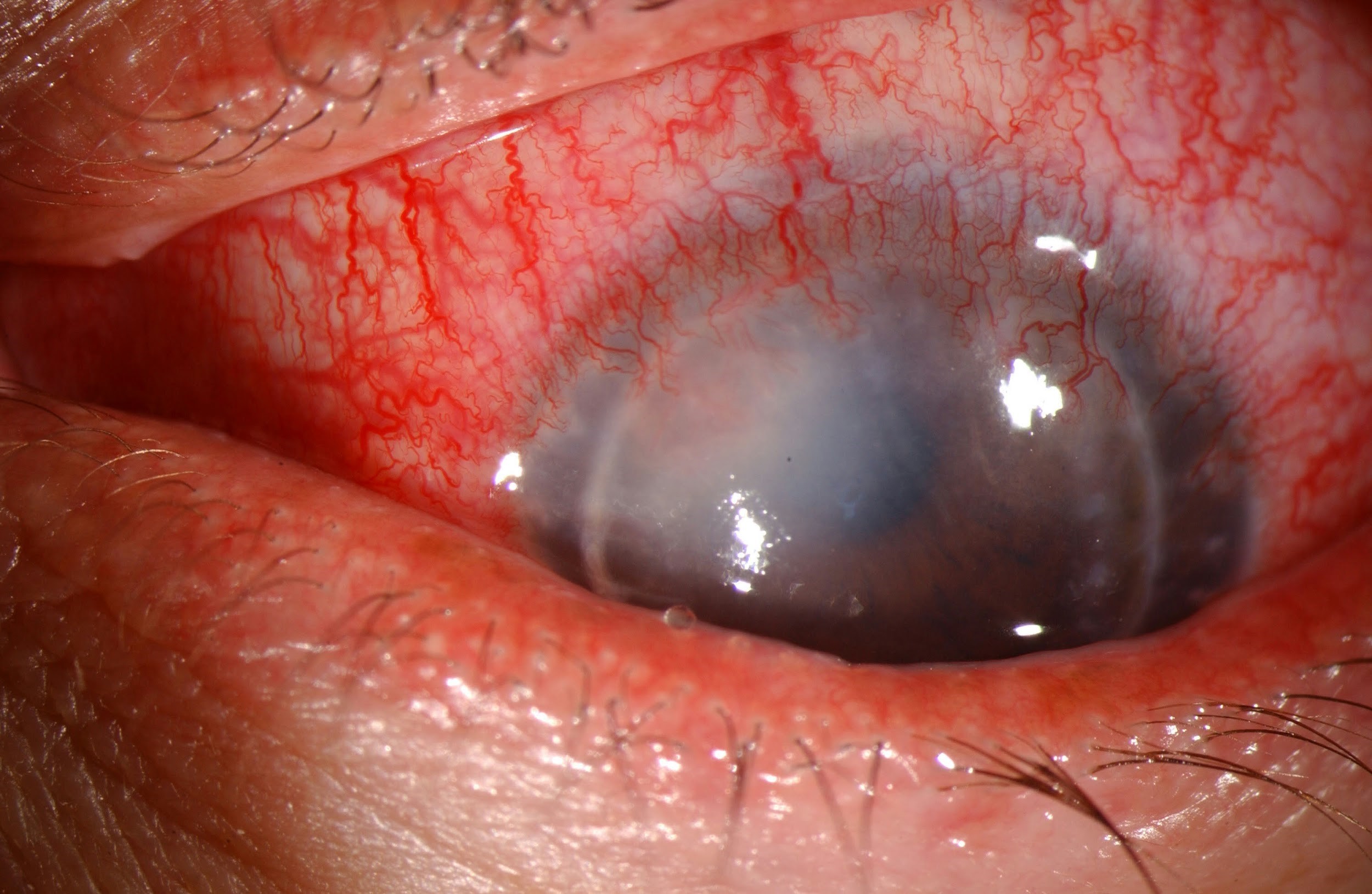
Figure 3 (right): Slit lamp photo of aggressive allograft rejection with active stromal vascularization and haze indicative of active graft rejection.

Figure 2 (left): Slit lamp photo of a penetrating keratoplasty with peripheral vascularization and stromal haze. The eye appears quiet and likely represents a chronic or past rejection.
Keywords/Main Subject: Keratoconus, Penetrating Keratoplasty, Transplant Rejection, Corneal Graft Rejection, Allograft Rejection, Corneal Vascularization, Immunosuppressives
Diagnosis: Corneal Transplant Rejection, Keratoconus
CASE
Chief Complaint: blurry vision of left eye for two weeks
History of Present Illness: A 35-year-old Caucasian female with bilateral keratoconus status post bilateral penetrating keratoplasty three years prior was referred for progressive blurry vision of the left eye for the past two weeks. Exam one year ago showed a healthy graft and clear cornea OU with visual acuity of 20/20 OD uncorrected and 20/20 OS corrected with a contact lens. The patient denied pain, discomfort, or discharge, stating only that the blurriness is “annoying.” No vision complaints OD. Using 1 drop of prednisolone acetate 1% once daily OU.
Past Ocular History: Keratoconus OU status post penetrating keratoplasty OU. Phacoemulsification with toric IOL for posterior subcapsular cataract OD, levator resection for ptosis OU, and a nuclear cataract OS currently stable under observation.
Medical history: FAP Gardner’s Syndrome
Family History: None
Social History: denies smoking, alcohol, illicit drugs
Medications: 1 drop prednisolone acetate 1% daily OU
Allergies: Morphine
Ocular Examination:
- Visual Acuity – best corrected with contact lens:
- OD – 20/25 +/-2
- OS – 20/200, 20/70 with pinhole
- Intraocular pressure (IOP by applanation):
- OD – 12 mmHg
- OS – 18 mmHg
- Pupils: No APD OU
- Slit lamp examinations:
- OD – cornea clear, penetrating keratoplasty, posterior chamber intraocular lens
- OS – cornea 3+ edema, superior rejection line, neovascularization 360 degrees, broken suture inferior
Assessment:
Corneal transplant rejection OS
Plan:
Prednisolone 1% every hour OS
Preservative free tears hourly OS
Follow-up in 2 weeks
CORNEAL ALLOGRAFT REJECTION DISCUSSION
Introduction:
Corneal graft transplant is the most widely practiced and successful type of solid organ transplantation in humans.1 Approximately 60,000 procedures are performed annually worldwide for diseases such as keratoconus, psuedophakic or phakic bullous keratopathy, trauma, infections, and corneal dystrophies or ectasias.1 It is associated with a high survival rate of 86% at 1-year post initial graft, largely attributed to the immune privilege of the eye.2 However, the 15-year graft acceptance rate declines to 55%, similar to survival rates in other forms of organ transplant.3 Graft rejection is one of the leading causes of corneal graft failure in the immediate and late postoperative period.1 Immune rejection and graft-related problems constitute the most important emergent presentations in graft patients. Long-term prophylactic use of topical steroids and immunosuppressive drugs can improve graft survival rate, but do not eliminate the risk, especially in “high-risk” recipients, and can be accompanied by side effects and potential toxicity.1 Novel biologic agents are showing promise in these patients unable to tolerate steroids.
Definition:
Corneal graft rejection is a reversible immune response against donor antigens. If signs of immunologic graft rejection do not clear within 2 months, the diagnosis of graft failure is made. Graft failure is the irreversible loss of graft clarity. It is important to rule out other common causes of loss of graft clarity before declaring failure. These include, but are not limited to infection, surgical trauma, glaucoma, and aging. Graft rejection is the most common cause of ultimate graft failure, accounting for >30% of cases.2
Pathophysiology:
The immune privilege of the cornea is maintained by the absence of blood vessels and lymphatics that deliver antigens to T cells in lymph nodes, scarcity of mature antigen presenting cells (APCs) in the central cornea, unusually low expression of major histocompatibility complex (MHC) antigens, and expression of the FAS ligand that induces apoptosis of stimulated Fas+ T cells.1 This privilege can be revoked by inflammation, infection, or trauma that induce neovascularization and lymphatic growth into the cornea; thus permitting APCs to enter the corneal stroma.1 Infection also induces pro-inflammatory cytokines that upregulate MHC antigen expression on corneal cells. Once the host immune system recognizes these foreign histocompatibility antigens on the cells of the corneal allograft, an immune cascade and response is initiated against these antigen, leading to eventual decompensation of the graft tissue.1 This rejection represents a form of delayed-type hypersensitivity response mediated by CD4+ T cells.2
Allograft rejection can affect one or more layers of the cornea (epithelium, stroma, and endothelium). The endothelium possesses minor regenerative properties and is a key player to maintaining corneal deturgescence.2 Thus, when >50% of the corneal endothelium is lost, graft rejection is likely to progress to graft failure.
Risk factors
Donor, host, and intraoperative factors influence graft rejection in corneal transplant recipients (Table 1). “High Risk” is defined as deep stromal vascularization of the host cornea of two or more quadrants, or a previous graft rejection in the affected eye.1
Table 1: Risk factors predisposing to graft rejection
| Donor
Factors |
· High antigenic load (depends on HLA/ABO compatibility between donor/host)
· Longer duration of storage of donor cornea (may reduce rejection) · Pretreatment of donor tissue with UV radiation (may reduce rejection by preventing activation of cytotoxic T cells) |
| Host
Factors |
· Vascularization of host cornea
· History of previously rejected graft (pre-sensitizes the host) · Ocular surface diseases (severe dry eye, chemical burns, radiation burns, ocular pemphigoid, Stevens-Johnson Syndrome, neuroparalytic disease) · Active keratitis · Pediatric patients (immune systemic of children is more active than adults)
|
| Intraoperative Factors | · Large/eccentric graft
· Synechiae at graft host junction · Penetrating grafts · Previous anterior segment surgical reconstruction · Bilateral graft · Suture removal (may trigger immune rejection) |
Clinical Signs and Symptoms:
Patients may be asymptomatic or may complain of increased blurry vision, redness, pain, irritation, or photophobia. Signs of graft rejection include:
- Stromal and/or epithelial edema
- Keratic precipitates (KPs) localized to the donor graft
- Corneal vascularization
- Stromal infiltrates
- Khodadoust line (separating immunologically damaged endothelium from unaffected endothelium)
- Elevated epithelial rejection line
- Krachmer spots (subepithelial infiltrates)
- Conjunctival injection
- Anterior chamber inflammation
Rejection can be classified based on corneal layer involvement (Table 2).1 Chronic focal endothelial rejection is the most common cause of graft rejection constituting 50% of cases. Epithelial rejection and stromal rejection represent roughly 2% and 1% of graft rejections, respectively.4
Table 2: Differentiating Features in Corneal Graft Rejection
| Epithelial | · Epithelial rejection line at the host graft junction
· Asymptomatic · No edema, keratic precipitates, or infiltrate |
| Stromal | · Circumferential limbal injection
· Patches of stromal infiltrate and haze · Stromal edema · Lymphocytes and plasma cells outside endothelial capillary wall |
| Endothelial | · Endothelial line
· Stromal and epithelial edema · Keratic precipitates on graft endothelium · Cell and flare possible, but difficult to visualize due to edematous cornea |
Adapted from Panda A, Vanathi M, Kumar A, et al. Corneal graft rejection. Survey of Ophthalmology. 2007; 52: 375-95.
Differential Diagnosis of Corneal Graft Rejection:
- Suture abscess or corneal infection
- Uveitis
- Epithelial downgrowth
- Recurrent herpetic keratitis
- Sterile or infectious endophthalmitis
- Increased IOP
Workup
Diagnosis is based on history and slit lamp examination. Important questions to be considered include: time since corneal transplantation, current eye medications, compliance with eye medications and postoperative follow-up, recent changes in topical steroid regimen, and inquiry into the initial indication for the corneal transplant. On slit lamp exam, inspect for endothelial rejection line, keratic precipitates, subepithelial infiltrates, edema, and cells in anterior chamber.
Prevention Practices and Immunosuppressive Agents:
Prevention can be subdivided into preoperative, intraoperative, and postoperative measures. Preoperatively, minimizing the antigenic difference between the host and donor tissue (tissue matching) and reducing the antigenic load of the donor tissue (UV light exposure) can help diminish the risk of rejection. Intraoperative measures of preventing immune-mediated allograft rejection are achieved by meticulous surgical techniques including good graft-host apposition and sterile suturing. Close follow-up monitoring for IOP, intact sutures, and compliance to immunosuppressive medications contribute to post-operative risk reduction.
Immunosuppressive medications play a fundamental role in the reduction of graft rejection. Current practice guidelines suggest “low risk” patients be put on long-term once daily prophylactic topical steroids (1% prednisolone drops), while “high risk” recipients adhere to a more stringent prophylactic regimen of long-term daily topical steroid plus a systemic immunosuppressive.1 Topical and oral steroids control the host immune system by preventing invasion by IL-1 and IL-6 producing macrophages and initiation of T-cell responses. Given the side effect profile of prolonged steroid use including cataract formation, glaucoma, and impaired wound healing, newer preventative therapeutics are becoming more widely available. Calcineurin inhibitors including cyclosporine (CsA), tacrolimus (FF-506), and mycophenolate mofetil (MMF) have been shown to be effectively substituted for steroids.5 Intraocular delivery of immunosuppressants in “high risk” rabbits was associated with reduced rate of graft rejection compared to those treated with topical or oral agents alone; supporting another potential route of prophylaxis.2 Novel biologic agents blocking receptors of TNF-a, VEGF, and CCL2 are also showing promise as prophylactic treatment in patients affected by high immune risk and corneal neovascularization.6 These agents work by reducing corneal inflammation, vascularization, angiogenesis, lymphangiogenesis; all factors common to graft rejection.2
Treatment
Despite prophylactic efforts, graft rejection may transpire. Management is aimed at reducing the active immune response. The likelihood of reversibility is largely dependent on the corneal layer affected. For epithelial and subepithelial acute rejections, which have a higher rate of reversibility, primary treatment involves topical steroids (1% prednisolone) six times per day along with preservative-free artificial tears that hydrate the ocular surface.7 Severe endothelial rejection requires hourly topical steroids in combination with systemic therapy (40 to 80 milligrams of oral prednisone daily, or 1-2 intravenous doses of 400 milligrams of methylprednisolone with or without subconjunctival betamethasone 3 milligrams in 0.5 milliliters).7 Careful monitoring for IOP and resolution of the inflammation should be assessed every 3-7 days until improvement is noted, at which point steroids may be slowly tapered and maintained at a long-term low dose.
Alternatives to Normal Corneal Tissue Grafts in “High Risk” Patients:
One alternative for patients with multiple failed corneal grafts is a Boston keratoprosthesis, an artificial cornea. This is a synthetically generated cornea FDA-approved for use in patients with severe corneal opacification and high risk of transplant failure. Donor corneal tissue is secured between a rigid polymethyl methacrylate optic front plate and back plate lined with holes to allow for communication with the aqueous for nutrition and hydration of the cornea. The plates are snapped together and sutured into the recipient eye, similar to a typical corneal transplant.8-9 A prospective case series of 141 cases across 17 centers reported visual acuity of 20/40 in 23% of patients and 20/200 in 57% of patients after keratoprosthesis placement.10 Failure for visual acuity improvement and post-operative complications included epithelial defects, stromal thinning, dellen formation, retroprosthetic membrane formation, retinal detachment, and development of glaucoma.2,11
Bioengineered corneal equivalents represent another possible option. These biosynthetic implants are equivalent to corneal stromal extracellular matrix and are based on chemically crosslinked collagen designed to function as regeneration templates. The idea is that regeneration of endogenous corneal layers and functional corneal nerves occur in the collagen matrix, thus hydrogel implants that mirror this natural cornea structurally may promote active regeneration of endogenous corneal epithelial and stromal cells.2 A recent 4-year follow-up clinical study provided strong evidence supporting high acceptance and adaptation of the hydrogel with improved visual acuity and central nerve ingrowth.12 The major limitation of this method resides in the fact that positive outcomes are limited to lamellar keratoplasty, in which host endothelium is still intact. This would not be helpful in patients requiring penetrating keratoplasty.
References:
- Panda A, Vanathi M, Kumar A, et al. Corneal graft rejection. Surv Ophthalmol. 2007;52:375-95.
- Yu T, Rajendran V, Griffith M, Forrester JV, Kuffova L. High-risk corneal allografts: a therapeutic challenge. World J Transplant. 2016;6:10-27.
- Williams KA, Esterman AJ, Bartlett C, Holland H, Hornsby NB, Coster DJ. How effective is penetrating corneal transplant? Factors influencing long-term outcome in multivariate analysis. Transplantation. 2006;81:896-901.
- Guilbert E, Bullet J, Sandali O, Basli E, Laroche L, Borderie VM. Long-term rejection incidence and reversibility after penetrating and lamellar keratoplasty. Am J Ophthalmol. 2013;155:560-69.
- Hill JC. Systemic cyclosporine in high-risk keratoplasty: long-term results. Eye (Lond). 1996;9:422-28.
- Fasciani R, Mosca L, Giannico MI, Ambrogio SA, Balestrazzi E. Subconjunctival and/or intrastromal bevacizumab injections as preconditioning therapy to promote corneal graft survival. Int Ophthalmol. 2015;35:221-7.
- Bagheri N, Wajda BN. The Wills Eye Manual: office and emergency room diagnosis and treatment of eye disease, 7th edition. Philadelphia: Lippincott Williams and Wilkin, 2017:98-99.Print.
- Ilhan-Sarac O, Akpek EK. Current concepts and techniques in keratoprosthesis. Curr Opin Ophthalmol. 2005;16:246-50.
- Birkholz ES, Goins KM. Bostom keratoprosthesis: an option for patients with multiple failed corneal graft. March 9, 2009; Available from: http://www.EyeRounds.org/cases/94-Boston-Keratoprosthesis-Failed-Corneal-Graft.htm
- Zerbe BL, Belin MW, Ciolino JB. Boston type 1 keratoprosthesis study group, results from the multicenter Boston Type 1 Keratoprosthesis study. Ophthalmol. 2006;113:1779.
- Ray S, Khan BF, Dohlman CH, D’Amico DJ. Management of vitreoretinal complications in eyes with permanent keratoprosthesis. Arch Ophthalmol. 2002; 120: 559–566.
- Fagerholm P, Lagali NS, Ong JA, Merrett K, Jackson WB, Polarek JW, Suuronen EJ, Liu Y, Brunette I, Griffith M. Stable corneal regeneration four years after implantation of a cell-free recombinant human collagen scaffold. Biomaterials. 2014; 35: 2420-27.
Faculty Approval by: Brian E. Zaugg, M.D.
Copyright: Charlotte L Marous © 2016. For further information regarding rights to this collection, please visit: http://morancore.utah.edu/terms-of-use/
Identifier: Moran_CORE_21656
Disclosure (Financial or other): The authors have no financial conflicts of interest.
UNDER REVIEW
Familial Exudative Vitreoretinopathy
Home / Pediatric Ophthalmology and Strabismus / Disorders of the Retina and Vitreous
Title: Familial Exudative Vitreoretinopathy
Author (s): Jeffrey Z. Kartchner, BS; Mary E. Hartnett, MD
Photographer: Unknown
Date: 07/20/2016
Keywords/Main Subjects: Familial exudative vitreoretinopathy, exudative retinal detachment, persistent fetal vasculature, retinopathy, leukocoria
Secondary CORE Category: Retina and Vitreous / Diseases of the Vitreous and Vitreoretinal Interface
Diagnosis: Familial Exudative Vitreoretinopathy
Format: Case presentation
History of Present Illness: A 4-month old boy born at full term after an uncomplicated pregnancy presented with exophoria and microphthalmia of the left eye, and also with right eye preference. He was seen by an outside pediatric ophthalmologist and diagnosed with leukocoria and probable persistent fetal vasculature (PFV) and referred to our retina service for surgery.
Past medical history was unremarkable. Family history was positive for mother with strabismus and maternal uncle with congenital cataract of unknown etiology.
Initial Examination: The patient’s visual acuity was “fix & follow” in both eyes. He had a mild afferent pupillary defect in the left eye, but none present in the right eye. His corneal diameter on the left side was 10mm, compared to 11mm on the right. External exam was otherwise normal bilaterally. Fundus exam of the right eye was normal, but no view was achieved on the left eye because of a dense retrolental membrane. A B-Scan ultrasound was performed, which showed a total retinal detachment with an open funnel. The decision was made to proceed with examination under anesthesia (EUA) with plans to perform a lensectomy and vitrectomy in the left eye for presumed PFV.
Clinical Course: The patient underwent EUA and was found to have an area of peripheral avascular retina in the right eye. Fluorescein angiography of this eye later showed peripheral avascular retina and leakage of the vessels at the junction of vascular and avascular retina consistent with stage 2A FEVR (Figure 1). The patient underwent lensectomy and vitrectomy in the left eye which revealed a retrolental membrane and a complete retinal detachment with a nasal exudative retinal fold, consistent with Stage 5 FEVR (Figure 2).
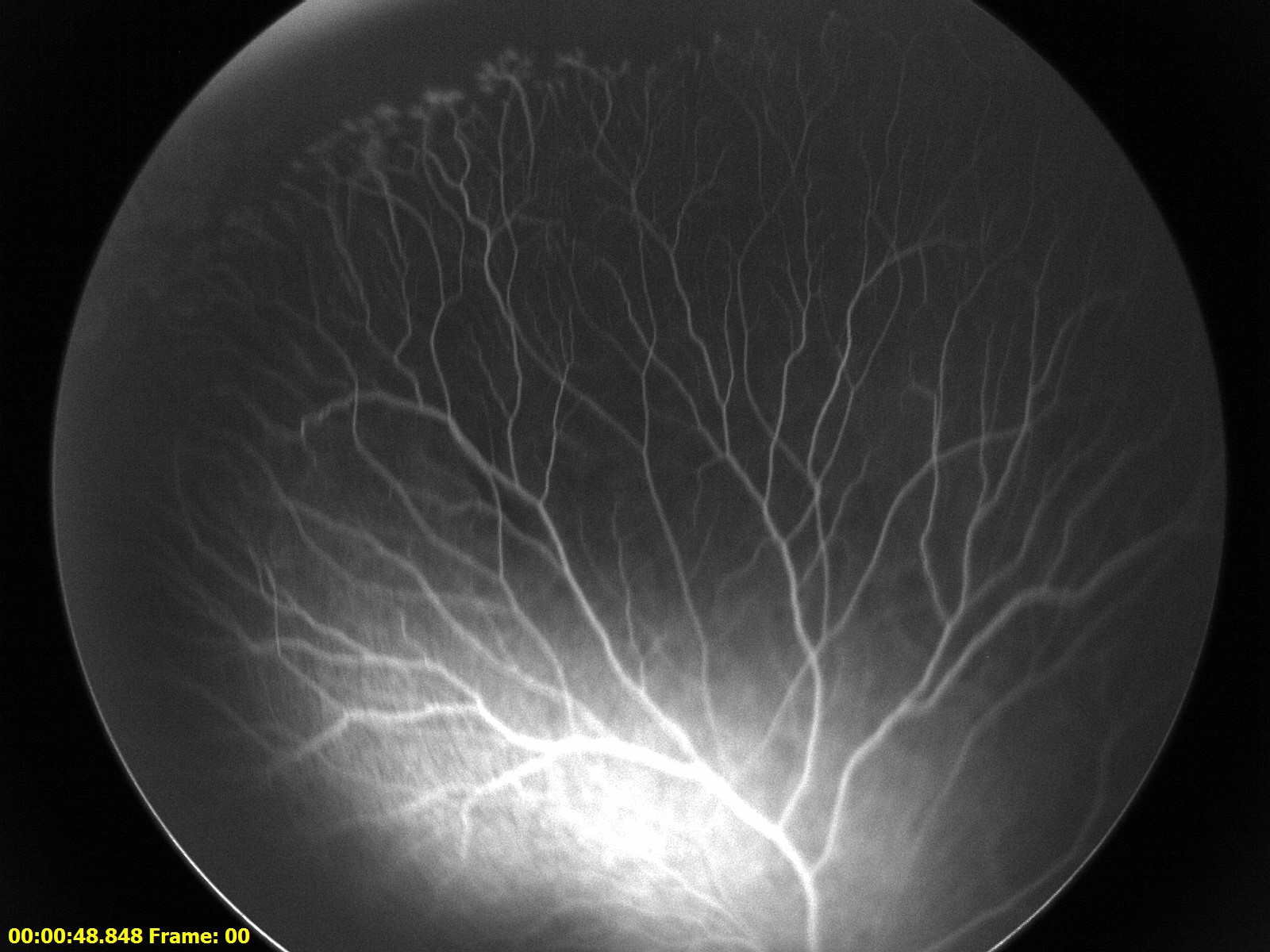
Figure 1: Fluorescein angiography (FA) of the right eye. There is an area of peripheral avascular retina with neovascular tufts along the border.
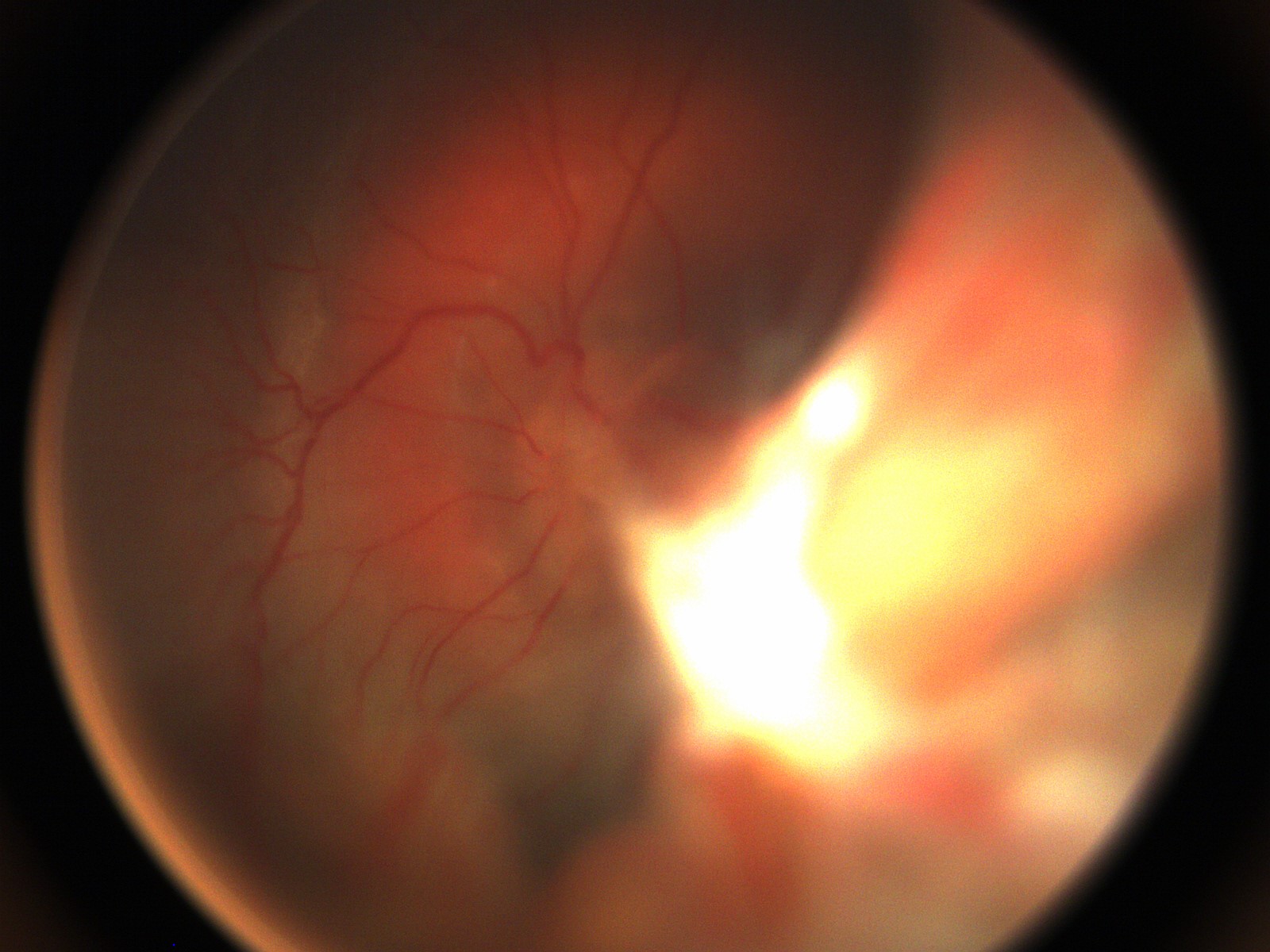
Figure 2: Fundus photography of the right eye following initial lensectomy-vitrecomy, demonstrating the nasal fold from the surgeon’s view and a circumferential subretinal band surrounding the optic nerve.
The patient underwent scatter photocoagulation of the avascular retina in the right eye (Figure 3). The patient subsequently underwent several additional EUAs and surgeries to drain subretinal fluid or release traction. Genetic studies revealed a heterozygous mutation of the FZD4 gene via the EyeGene research study.

Figure 3: FA of the right eye. Scatter photocoagulation has been performed to include the avascular retina and neovascularization in its entirety.
Current Exam: At age 21-months the patient’s visual acuity in the right eye is 20/32 by Allen acuity cards and light reactive in the left eye. There is a 3+ afferent pupillary defect in the left eye. Disease in the right eye has been stable after scatter photocoagulation. The left eye shows reattachment of the retinal detachment with resolving subretinal exudates and the persistent subretinal band and nasal fold (Figure 4). Current management includes regular monitoring and maximizing his visual outcome with consideration of the aphakic correction of the left eye.

Figure 4: Fundus photography of the left eye. Intra-retinal cholesterol crystals remain after some resolution of exudates. A sub-retinal band with persistent exudates is observed extending anteriorly.
Discussion:
FEVR is a genetically inherited disease with multiple modes of inheritance, including autosomal dominant, autosomal recessive, and X-linked. Expressivity is variable, such that it is common for patients to present with widely different phenotypes, even between eyes in the same individual. Up to 58% of relatives of patients diagnosed with FEVR have asymptomatic clinical findings1. Mutations in FZD4, LRP5, NDP and TSPAN12, members of the Wnt signaling pathway, are implicated in about 50% of cases. Newly discovered mutations in ZNF408 have also been shown to lead to disease2.
Genetic mutations lead to incomplete vascularization of the peripheral retina in full-term infants that may progress to neovascularization. The disease appears similar to acute retinopathy of prematurity (ROP). Exudative retinal detachment, retinal folds, macula ectopia, fibrous bands, and tractional retinal detachments also occur with FEVR progression. Studies have been performed evaluating the location of retinal folds in children with FEVR3,4. It was shown that patients with retinal folds extending from the posterior pole to the lens present in such a way that the diagnosis of FEVR can be difficult to distinguish from PFV, as was the case in the current patient presentation. It is, therefore, imperative to perform EUA with careful examination of the contralateral eye for any signs of FEVR.
Management of FEVR includes early screening in suspected cases, with prompt laser photocoagulation therapy or cryotherapy to any avascular retina and neovascularization. Retinal detachments are managed surgically, with frequent follow-up for monitoring of repeat detachments. Recent studies have been performed evaluating the efficacy of anti-VEGF agents in the treatment of FEVR. While initial results can be promising, the long-term therapy in these patients did not provide sustained positive outcomes5. Limitations to research regarding FEVR include the small patient population and wide variability of expressivity between patients.
References:
1. Trese MD et al. High prevalence of peripheral retinal vascular anomalies in family members of patients with familial exudative vitreoretinopathy. Ophthalmology. 2014;121(1):262-8.
2. Collin RW, Nikopoulos K, Dona M, Gilissen C, Hoischen A, Boonstra FN et al. ZNF408 is mutated in familial exudative vitreoretinopathy and is crucial for the development of zebrafish retinal vasculature. Proc Natl Acad Sci USA. 2013; 110: 9856–9861.
3. Robitaille JM et al. Phenotypic Overlap of Familial Exudative Vitreoretinopathy (FEVR) with Persistent Fetal Vasculature (PFV) Caused by FZD4 Mutations in two Distinct Pedigrees. Ophthalmic Genet. 2009;30(1):23-30
4. Trese MD et al. Clinical Presentation of Familial Exudative Vitreoretinopathy. Ophthalmology. 2011;118(4):2070–2075.
5. Henry CR. Long-term follow-up of intravitreal bevacizumab for the treatment of pediatric retinal and choroidal diseases. J AAPOS. 2015 Dec;19(6):541-8.
Faculty Approval by: Mary E. Hartnett, MD
Copyright statement: Copyright ©2015. For further information regarding the rights to this collection, please visit: Terms of Use to copyright information page on Moran CORE
Identifier: Moran_CORE_21639
Disclosure (Financial or other): None
UNDER REVIEW
Central Serous Chorioretinopathy – Case Report
Home / Retina and Vitreous / Choroidal Disease
Title: Central Serous Chorioretinopathy
Author: Sravanthi Vegunta, Eileen S. Hwang, Mary E. Hartnett
Photographer: Mel Chandler
Date: 08/05/2015
Keywords/Main Subjects: Central serous chorioretinopathy; Scotoma; Metamorphopsia; Retinopathy; Corticosteroid use; Smoke stack
Diagnosis: Central serous chorioretinopathy
Brief Description: History of Present Illness: The patient was a 46 year old female with a history of hypothyroidism, depression and seasonal allergies who presented 5 weeks after the sudden onset of a floaters, a paracentral scotoma and distortion in her left eye. At first, her central vision was primarily affected, but shortly before her presentation in our clinic, the affected area spread to include an area to the right as (Figure 1). She denied visual problems with her right eye.
Her medical history was significant for the use of intranasal steroid spray for seasonal allergies. She had stopped this a few weeks prior to presentation after a visit to an outside ophthalmologist.

Figure 1: Amsler grid test of the left eye revealed a central grey area and a superior area of distortion.
Initial examination: The patient’s visual acuity with correction was 20/20 in the right eye and 20/60 in the left eye. Intraocular pressure was 16 mmHg in the right eye and 16 mmHg in the left eye. She did not have a relative afferent pupillary defect. Confrontation visual fields and extraocular motility were intact. Anterior segment slit lamp examination was normal in both eyes. On fundus examination, both optic nerves were normal in appearance with a cup-to-disc ratio of 0.3 in the right eye and 0.2 in the left eye. The macula of her right eye was normal with a good foveal reflex. Her left macula had an area of pigment near the fovea (Figure 2) and the retina appeared elevated in the central macula, consistent with subretinal fluid (Figure 3). The retinal vasculature and periphery were normal in both eyes.

Figure 2: Color fundus photography. A) The right macula and fovea appear normal. B) In the left eye, the foveal reflex appears yellow and blunted. There are parafoveal pigmentary changes. There is an area of retinal elevation consistent with subretinal fluid in the central retina.
Clinical Course: Patient underwent optical coherence tomography (OCT; Figures 3 and 4) and fluorescein angiography (FA; Figure 6) of each eye.

Figure 3: Left eye OCT demonstrating subretinal fluid in the central macula.

Figure 4: Left eye infrared image showing a hyporeflective area in the central macula corresponding to the area of subretinal fluid.

Figure 5: Fluorescein angiography of the left eye. There are window defects and late phase leakage from a point in the inferior macula toward the fovea in a smoke stack configuration.
The patient was diagnosed with central serous chorioretinopathy (CSCR) and informed that her visual changes were likely to improve without intervention. Information was provided to the patient regarding the limited quality data for treatment of CSCR with spironolactone, rifampin, epleronone, and low dose aspirin. Low dose aspirin was recommended to the patient since there was a controlled study supporting its use, and the risks were felt to be relatively benign.
Discussion:
CSCR is characterized by a build up of subretinal fluid in the macula caused by abnormalities of the choroidal circulation.1 Fluid leaks from the choroidal circulation and passes through hyperpermeable areas of the retinal pigment epithelium (RPE), accumulating in the subretinal space. 2
While the specific cause of CSCR is not well understood, some systemic risk factors have been associated with CSCR. In particular, corticosteroid administration and stressful events (presumably associated with high endogenous corticosteroid levels) are associated with the development of CSCR.2 The patient described in this case report was using intranasal steroids, which have specifically been associated with CSCR in addition to systemic, intraarticular, and topical steroids.
CSCR occurs most often in males between 20 and 50 years of age. It usually presents with acute onset of unilateral metamorphopsia, blurred vision and a relative scotoma. Patients can also experience micropsia, impaired dark adaptation, and color desaturation. Presenting visual acuity ranges from 20/15 to 20/200 with an average of 20/30. On fundus examination, there is often an elevation of the neurosensory retina in the central macula due to subretinal fluid. It is important to perform careful inspection of the fundus to exclude conditions such as optic nerve pit, age-related macular degeneration, polypoidal choroidal vasculopathy, uveitis, and intraocular tumor which can also cause subretinal fluid. OCT can be used to identify and follow the amount of subretinal fluid.1, 2 FA reveals leakage of dye from a focal choroidal/RPE defect which collects in the subretinal space. This usually occurs in an ink-blot pattern in which the spot of hyperfluorescence secondary to leakage spreads concentrically, but in 10-15% of cases, the dye can spread linearly in a smoke stack configuration, as demonstrated in the imaging from the patient described here.
Visual disturbances often resolve spontaneously in a few months, although recurrence is common and chronic CSCR can occur. Some patients experience permanent visual changes. If the subretinal fluid fails to resolve with observation alone, photodynamic therapy (PDT) may be performed to hasten subretinal fluid resorption. There is no evidence that PDT improves final visual outcomes, but since photoreceptor atrophy begins as early as 4 months after onset, there may be a theoretical a long term benefit to treatment if the fluid persists for more than 3 months. However, PDT is not without significant risk of vision loss and secondary CNV. The use of half-dose verteporfin and a 10 minute time interval between infusion and laser application may reduce these risks while still providing efficacious treatment of the abnormal choroidal vasculature.
In additional to PDT, several other treatment options for CSCR have been studied. However, studies with large sample sizes and prospective, controlled design are lacking. Studies of the efficacy of bevacizumab and ranibizumab therapies have shown significantly improved retinal thickness and visual acuity in the first 3 months following treatment, but this improvement is not sustained beyond 6 months.3-7
Medications that inhibit mineralocorticoid production or antagonize the mineralocorticoid receptor have recently been studied as potential treatments for CSCR. Zhao et al.8 demonstrated efficacy of eplerenone in a CSCR animal model, and a small pilot study of 13 human patients showed promise.9. There are a handful of ongoing clinical trials for eplerenone, which is an FDA-approved medication used in the treatment of congestive heart failure.
Caccavale et al.10 studied the efficacy of aspirin for CSCR treatment with the rationale that aspirin may correct abnormalities of the choroidal vasculature and reduce serum levels of plasminogen activator inhibitor 1 (PAI-1), elevated levels of which have been found in patients with CSCR.11, 12 Caccavale et al. conducted a prospective trial in which patients treated with six months of 100 mg aspirin demonstrated improved visual acuity compared to historic controls. Significant improvements in visual acuity were present at one month and three months, and persisted to twelve months.
In the case of the patient described in this case report, she was eagerly seeking some kind of treatment. PDT was not recommended because at one month after onset, the risk of vision loss from PDT was not justified in a disease with a 90% spontaneous resolution rate. Eplerenone was considered, but excluded because of the need for monitoring serum potassium. The patient was started on low dose aspirin since there was some evidence supporting its efficacy, and the risks of this treatment were relatively low.
Series: Case Report 2015
References:
- Kanski J, Bowling B. Clinical Ophthalmology, 7 ed. United Kingdom: Elsevier Health Sciences, 2011.
- Ryan S, Schachat A, Wilkinson C, Hinton D, Sadda S, Wiedemann P. Retina, 5 ed. United Kingdom: Elsevier Health Sciences, 2013.
- A randomized trial comparing intravitreal triamcinolone acetonide and focal/grid photocoagulation for diabetic macular edema. Ophthalmology 2008;2008 Sep;115:1447-9.
- Aydin E. The efficacy of intravitreal bevacizumab for acute central serous chorioretinopathy. J Ocul Pharmacol Ther 2013;29:10-3. doi: 10.1089/jop.2012.0072. Epub 2012 Aug 27.
- Lim JW, Ryu SJ, Shin MC. The effect of intravitreal bevacizumab in patients with acute central serous chorioretinopathy. Korean J Ophthalmol 2010;24:155-8. doi: 10.3341/kjo.2010.24.3.155. Epub 2010 Jun 5.
- Artunay O, Yuzbasioglu E, Rasier R, Sengul A, Bahcecioglu H. Intravitreal bevacizumab in treatment of idiopathic persistent central serous chorioretinopathy: a prospective, controlled clinical study. Curr Eye Res 2010;35:91-8. doi: 10.3109/02713680903428306.
- Park SU, Lee SJ, Kim M. Intravitreal anti-vascular endothelial growth factor versus observation in acute central serous chorioretinopathy: one-year results. Korean J Ophthalmol 2014;28:306-13. doi: 10.3341/kjo.2014.28.4.306. Epub 2014 Jul 22.
- Zhao M, Celerier I, Bousquet E, et al. Mineralocorticoid receptor is involved in rat and human ocular chorioretinopathy. J Clin Invest 2012;122:2672-9. doi: 10.1172/JCI61427. Epub 2012 Jun 11.
- Bousquet E, Beydoun T, Zhao M, Hassan L, Offret O, Behar-Cohen F. Mineralocorticoid receptor antagonism in the treatment of chronic central serous chorioretinopathy: a pilot study. Retina 2013;33:2096-102.
- Caccavale A, Romanazzi F, Imparato M, Negri A, Morano A, Ferentini F. Low-dose aspirin as treatment for central serous chorioretinopathy. Clin Ophthalmol 2010;4:899-903.
- Yamada R, Yamada S, Ishii A, Tane S. [Evaluation of tissue plasminogen activator and plasminogen activator inhibitor-1 in blood obtained from patients of idiopathic central serous chorioretinopathy]. Nihon Ganka Gakkai Zasshi 1993;97:955-60.
- Iijima H, Iida T, Murayama K, Imai M, Gohdo T. Plasminogen activator inhibitor 1 in central serous chorioretinopathy. Am J Ophthalmol 1999;127:477-8.
Identifier: Moran_CORE_21271
Copyright statement: Copyright 2015. Please see terms of use page for more information.