
Parry-Romberg Syndrome
Home / Orbit, Eyelids, and Lacrimal System / Periocular Malpositions and Involutional Changes
Title: Parry-Romberg Syndrome Case Report
Author: Rebekah Gensure, PhD, 4th Year Medical Student, Rutgers Robert Wood Johnson Medical School; Laura Hanson, MD, Neuro-Ophthalmology Fellow, John A. Moran Eye Center; Kathleen Digre, MD, John A. Moran Eye Center
Photographer: James Gilman
Date: July 20, 2015
Moran CORE: Orbits, Eyelids, and Lacrimal System/Periocular Malpositions and Involutional Changes/Involutional Periorbital Changes
Keywords/Main Subjects: Parry-Romberg Syndrome, hemifacial atrophy
Diagnosis/Differential Diagnosis: Parry-Romberg Syndrome, post traumatic fat atrophy, hemifacial microsomia (first and second branchial arch syndrome), Goldenhar’s syndrome
Brief Description of Case:
HPI:
A 27-year-old female patient presented with a long history of facial asymmetry and right tongue atrophy. She was diagnosed with Parry-Romberg syndrome 7 years ago, at the age of 20. At the time of her initial diagnosis at an outside institution, the patient report experiencing significant facial pain and wasted facial appearance that had been present for many years and had gone undiagnosed until that point. Presently, the patient is status-post surgical repair (hemifacial fat grafting) with a satisfactory cosmetic result.
The patient also has a history of migraine headache. At the time of the most recent visit, the patient reported improvement in migraine headaches with no preventative medications currently. Headaches have been less frequent (approximately 1 every 2 weeks) and pain rating no worse than 5/10. She also reports episodic ptosis, which appears to be related to migraine and menstrual cycle.
Other ocular history includes a history of treated amblyopia secondary to accommodative esotropia and is still in spectacle correction.
Exam: OCULAR:
Best corrected visual acuities: 20/20 OD and 20/20 OS.
Pupils: 3mm OU light, 7 mm OU dark; briskly reactive OU with no RAPD EOM: -½ OD on right gaze; Orthotropic at distance; exophoria at near Exophthalmometry: 13 mm OD, 16 mm OS
Color Vision: 10/10 OU Ishihara
Stereo Vision: +Fly, 3/3 animals, 7/9 circles IOP: 16 mm Hg OD & OS.
VF: Full OU
SLE: Anterior segment within normal limits
Fundus: Within normal limits; C/D ratio 0.1 OD, 0.2 OS Refraction: OD +2.50 sphere, +0.75 cylinder at axis 25
OS +1.50 sphere, +1.50 cylinder at axis 130
NEURO: Completely normal neurological examination except for the facial asymmetry.
Discussion:
Hemifacial atrophy, also known as Parry-Romberg syndrome, is characterized by a slow progressive deterioration (atrophy) of the skin and subcutaneous tissue structures on half of the face [1]. As it is described by Parry, Henoch and Romberg in the early 19th century, there is wasting of the subcutaneous fat with or without atrophy of adjacent skin, bone, and cartilage [2- 3]. The condition is typically insidious in onset, and progression is variable. In some cases, atrophy may halt before the entire hemi-face is involved but with residual disability [4]. In mild cases, there may be only minor cosmetic effects without any disability.
Because of the relative rarity of this condition, associated clinical conditions have mostly been identified through case reports. For example, in 1985, Sagild and Alving reported a case associating hemiplegic migraine with hemifacial atrophy [5]. Seizures are also commonly reported to co-occur with hemifacial atrophy, particularly contralateral simple partial or generalized seizures [6]. Additionally, Parry-Romberg syndrome has sometimes been associated with localized scleroderma, although this association remains controversial.
Long-term progression of the condition has not been well documented; however, one interesting case report followed several patients over time, including one patient who was followed for over 43 years [7]. For this particular long-term follow-up patient, progression of facial atrophy appeared to progress until age 15 but then slow or stop until age 23, at which point new onset hyperreflexia of the contralateral lower extremity was noted. Over the years, the facial atrophy remained apparently stable, although his neurological function gradually declined; by age 58, he demonstrated wide-based gait with absent plantar and tendon reflexes, mildly diminished pain and temperature sensation, end-position nystagmus, and difficulty with heel-to-shin and tandem testing.
Treatment options are limited for patients diagnosed with Parry-Romberg hemifacial atrophy. Currently, there are no known therapies that will stop progression of the disease.
Reconstruction has been utilized, with variable results depending on the timing of the intervention. For the best results possible, timing of surgery should be strategized according to when the disease appears to have exhausted its course and facial growth is completed [4].
Images or Video:
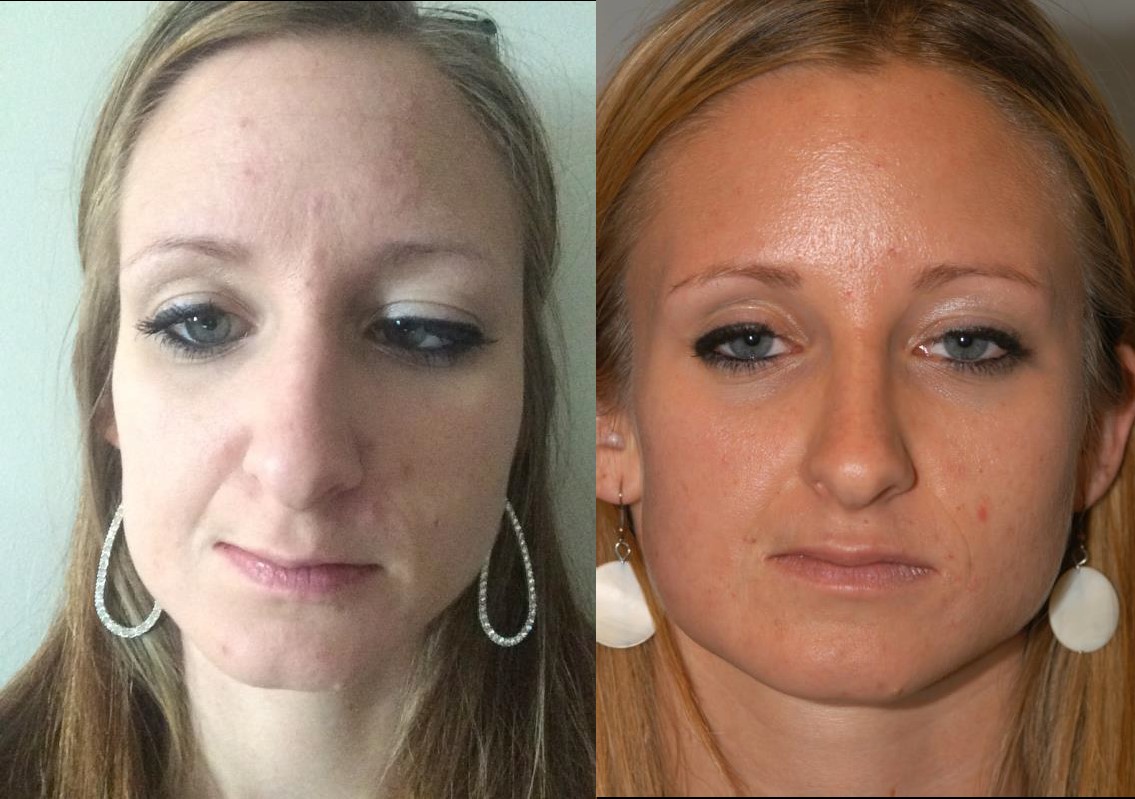
Figure 1 a): Right hemifacial atrophy at baseline in patient previously diagnosed with Parry- Romberg syndrome; b): Patient with Parry-Romberg syndrome with history of right hemifacial atrophy, status post fat grafting, with satisfactory cosmetic result. (Photographs courtesy of the patient)

Figure 2: Tongue hemiatrophy in patient with diagnosed Parry-Romberg syndrome. (Photograph by James Gilman)

Figure 3: Right enophthalmos observed in patient with Parry-Romberg syndrome with right hemifacial atrophy. Hertel measurements indicated posterior displacement of 3 mm on the affected side (right) compared to the unaffected (left) side. (Photographs by James Gilman)
Summary of the Case:
The patient is a 27-year-old woman with Parry-Romberg syndrome with hemifacial atrophy, status-post reconstructive surgical repair with a satisfactory cosmetic result. Overall, the patient is quite stable, with no major new changes in facial structure visible on external exam as compared to prior exams. Based on the apparent stability of the disease process and satisfaction of the patient with her appearance, the patient was recommended to return to clinic only for yearly follow-up or sooner as needed.
References:
- Esan T and Olusile Hemifacial Atrophy: A Case Report And Review Of Literature. The Internet Journal of Dental Science. 2003. 1(1).
- Parry Collections from the unpublished medical writings of the late Caleb Hillier Parry, M.D., F.R.S. 1825 London: Underwoods. 478–80.
- Romberg, MH; Henoch, EH (1846). Krankheiten des nervensystems (IV: Trophoneurosen). Klinische ergebnisse (in German). Berlin: Albert Förstner. 75–81.
- NINDS Parry-Romberg Information Page [Internet]. Bethesda: Office of Communications and Public Liaison, National Institute of Neurological Disorders and Stroke, National Institutes of Health; January 25, Available from: http://www.ninds.nih.gov/disorders/parry_romberg/parry_romberg.htm
- Sagild JC and Alving Hemiplegic migraine and progressive hemifacial atrophy; June 1985; 17(6): 620.
- Wolf SM and Verity Neurological complications of progressive facial hemiatrophy. J Neurol Neurosurg Psychiatry. 1974 Sep; 37(9): 997–1004.
- Asher SW and Berg Progressive hemifacial atrophy: Report of three cases, including one observed over 43 years, and computed tomography findings. Arch Neurol. 1982; 39: 44-46.
Faculty Reviewer: Griffin Jardine, MD
Copyright statement: Copyright 2017. Please see terms of use page for more information.