
Medulloepithelioma
Home / Pediatric Ophthalmology and Strabismus / Diseases of the Cornea, Anterior Segment and Iris
Title: Medulloepithelioma in an otherwise healthy newborn
Authors: Taylor Brady, MSIV – University of Utah School of Medicine; Griffin Jardine, MD
Photographers: Griffin Jardine, MD; Roger Harrie, MD
Date: 8/3/20
Images:

Figure 1: Medulloepithelioma in an otherwise healthy newborn. This 2-month-old female presented with an irregular iris border in the inferonasal quadrant. Note the ectropion uveae present in the image that is commonly seen in these tumors. (Credit: Dr. Griffin Jardine, MD)

Figure 2: Ultrasound A-scan of a pediatric patient with medulloepithelioma. The increased signaling posterior to the cornea and iris shows the location of the ciliary body lesion. (Credit: Dr. Roger Harrie, MD)

Figure 3: Ultrasound B-scan of a pediatric patient with medulloepithelioma. Note the small, hypoechoic foci found within the lesion itself. These foci demonstrate locations of differentiated tissues commonly found in teratoid medulloepithelioma. (Credit: Dr. Roger Harrie, MD)
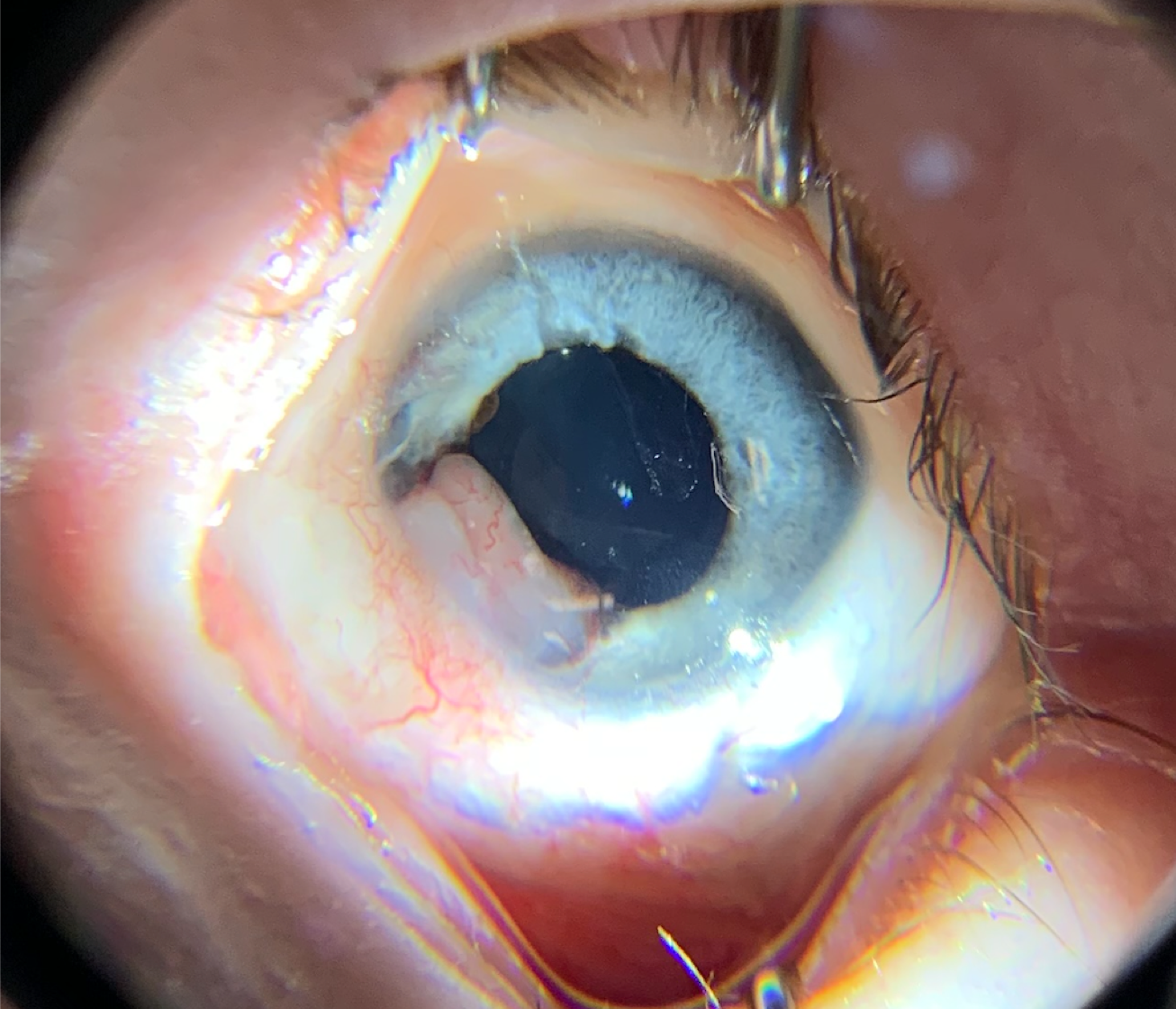
Figure 4: Two-year follow up image of the patient presented in this case. She was treated with plaque-radiotherapy. There has been no progression of the medulloepithelioma since treatment began at 6-months of age. Note the radiation-induced cataract partially visible in the lens. (Credit: Dr. Griffin Jardine, MD)
Keywords/Main Subjects: Medulloepithelioma, intraocular tumor, pediatric cancer, radiation therapy
Diagnosis: Medulloepithelioma
A 2 month-old female, who was otherwise healthy, presented with an irregular iris border ofthe left eye. Examination under anesthesia and ocular ultrasound was performed which elicited the diagnosis of medulloepithelioma.The medulloepithelioma was found to be relatively small at approximately 3 clock hours located in the inferonasal quadrant. There was no evidence of glaucoma or lens subluxation. The patient underwent a 5-month course of plaque-radiotherapy beginningat age 6-months.In order to place the radio-plaque, two extraocular muscles had to be shifted and were not reinserted at the original insertion. The patient developed strabismus and has subsequently undergone two strabismus surgeries. She has also developed a radiation-induced cataract of the left eye. As a consequence, she developed multifactorial amblyopia in the left eye which has been treated with glasses and 2 hours/day patching.
Now at 2-years-old, she has not had progression of the medulloepithelioma. She is undergoing close follow-up to ensure that the medulloepithelioma remains stable.
Epidemiology:
Medulloepithelioma is a rare intraocular cancer, so rare in fact, that incidence is difficult to quantify. 75-90% of intraocular medulloepitheliomas present in the first decade of life, however, there are reported cases of new medulloepitheliomas presenting in patients as late as in their 6th decade.
The rarity of medulloepithelioma decreases its likelihood of being caught early and/or increases the likelihood that it is misdiagnosed. This often leads to significant progression of the disease, increased treatment morbidity and worse prognosis.
Histopathology:
Medulloepithelioma arises from the non-pigmented ciliary epithelium. The two main classifications are teratoid and non-teratoid. These are further classified into benign or malignant, however, nearly 90% are malignant or have malignant potential regardless of their initial classification. Non-teratoid medulloepithelioma (previously referred to as “diktyoma”) contains cells which resemble ciliary epithelium. Teratoid medulloepithelioma often have diverse cell origins and can present with cartilaginous, neural or skeletal muscle tissue within the tumor.
Typical presentation:
Patients typically present with a clear to flesh-toned mass arising from the ciliary body. A lens colobomais commonly present because of congenital absence of zonulesin the area of the ciliary body where the tumor is located (typically inferotemporal).
Secondary signs at presentation may include presence of a cyclitic membrane, glaucoma due to the lesion causing angle closure, lens subluxation when there is mass effect displacing the lens, ectropion uveae and leukocoria.
Evaluation/Diagnosis:
Diagnosis of medulloepithelioma is made clinically with imaging playing a large role, especially ultrasound bio-microscopy. It is important to avoid intraocular biopsy of these tumors with fine needle aspiration because of risk of hemorrhage and/or seeding the tumor in other areas of the globe.
Treatment:
The mainstay of treatment for medulloepithelioma is enucleation, especially if the tumor is large(greater than 3-4 clock hours), is causing intraocular issues like glaucoma or lens subluxation, or has significant global involvement. If caught earlier, other treatment options are available including plaque-radiotherapy or local resection.
Prognosis:
Medulloepithelioma has a low histological metastatic risk compared to other intraocular pediatric cancer, namely retinoblastoma. Despite this lower risk, medulloepithelioma’s tendency to be diagnosed later in the course makes it more likely to have metastatic involvement. Even so, 5-year survival rates after enucleation are between 90-95%.
References:
- Cai S, Zhao W, NieX, et al. Multimorbidity and Genetic Characteristics of DICER1 Syndrome Based on Systematic Review.Journal of pediatric hematology/oncology.2017;39(5):355-361.
- Finger PT, Harbour JW, Karcioglu ZA. Risk factors for metastasis in retinoblastoma.Surv Ophthalmol. 2002;47(1):1-16.
- Moran Eye Center. (2020). Intraocular tumors –melanocytic. MoranCore. https://morancore.utah.edu/section-04-ophthalmic-pathology/tumors/
- Ortiz MV, Dunkel IJ. Retinoblastoma.J Child Neurol. 2016;31(2):227-236.
- Sadiq MA, Ramasubramanian A. (2020, July 11). Medulloepithelioma. American Academy of Ophthalmology. https://eyewiki.aao.org/Medulloepithelioma
- Shah PK, Meeralakshmi P, Shanthi R, Saravanan VR, Kalpana N, Narendran V. Pigmented ciliary body medulloepithelioma in a newborn infant.Oman J Ophthalmol. 2017;10(3):257-258.
- Shields JA, Shields CL. Intraocular Tumors. Second Edition. Lippincott Williams & Wilkins. 2008.
- Shields JA, Eagle RC Jr, Shields CL, Potter PD. Congenital neoplasms of the nonpigmented ciliary epithelium (medulloepithelioma).Ophthalmology. 1996;103(12):1998-2006.
- Tadepalli SH, Shields CL, Shields JA, Honavar SG. Intraocular medulloepithelioma -A review of clinical features, DICER 1 mutation, and management.Indian J Ophthalmol. 2019;67(6):755-762.
Faculty Approval by: Griffin Jardine, MD
Copyright Statement: Taylor Brady, ©2020. For further information regarding the rights to this collection, please see terms of use page.