
Leukocoria (in children)
Home / Basic Ophthalmology Review / Pupillary Exam
Title: Leukocoria (in children)
Author: Spencer Fuller, MSIV – UC San Diego School of Medicine, MPH
Definition: In contrast to the normal red reflex, leukocoria is defined as a yellow, pale, white, or otherwise abnormal reflection of light observed in the pupil of one or both eyes.
Presentation: The asymmetric “white pupil” is either caught by family members (often in photos with asymmetric red reflexes from the flash) or incidentally by a practitioner on routine direct ophthalmoscopy. Every well child check—especially the newborn baby check in the nursery—should include an examination of the pupils. Patients in whom leukocoria is observed should be promptly referred to an ophthalmic specialist for diagnosis and management.
Differential Diagnosis:
The differential diagnosis of leukocoria in children is broad and includes hereditary, developmental, inflammatory, neoplastic and miscellaneous conditions [1]:
- Strabismus – a common pediatric problem, ocular misalignments can cause asymmetric red reflex testing [see American Academy of Pediatrics (AAP) insert below]. Prompt referral of strabismus to a pediatric ophthalmologist is important to prevent amblyopia or poor visual development in the misaligned eye.
- Anisometropia – difference in refractive errors or prescriptions can cause an asymmetric red reflex where on eye is dimmer than the other—otherwise known as the “Bruckner test.”
- Retinoblastoma – the most common pediatric ocular malignancy, occurs primarily in children aged 18-24 months of age but can be much younger in those at higher risk. Retinoblastoma has been estimated to account for as much as 50% of leukocoria cases in United States.

This patient with leukocoria eventually was diagnosed with Retinoblastoma and underwent enucleation.
Jordan, Michael (2014). 2 year Old with Leukocoria. Moran Eye Center Grand Rounds http://morancore.utah.edu/section-06-pediatric-ophthalmology-and-strabismus/case-2-year-old-with-leukocoria/
- Congenital cataract – develops from numerous processes (i.e. infectious, metabolic, genetic) and can be either unilateral or bilateral. These can cause irreversible vision loss within a matter of weeks to months—prompt recognition, referral and surgical treatment is vital.
- Retinopathy of prematurity (ROP) – the most common cause of blindness in children in the United States, ROP occurs in premature (gestational age < 30 weeks) or underweight (< 1500 grams) babies as a result of abnormal retinal vessel development. Retinopathy develops due to irregular growth of retinal blood vessels that can lead to bilateral blinding retinal detachments. Thanks to an increased understanding of supplemental oxygen regulation in the NICU as well as ROP progression most cases are caught and treated. ROP patients are regularly followed by a pediatric ophthalmologist or retinal specialist.
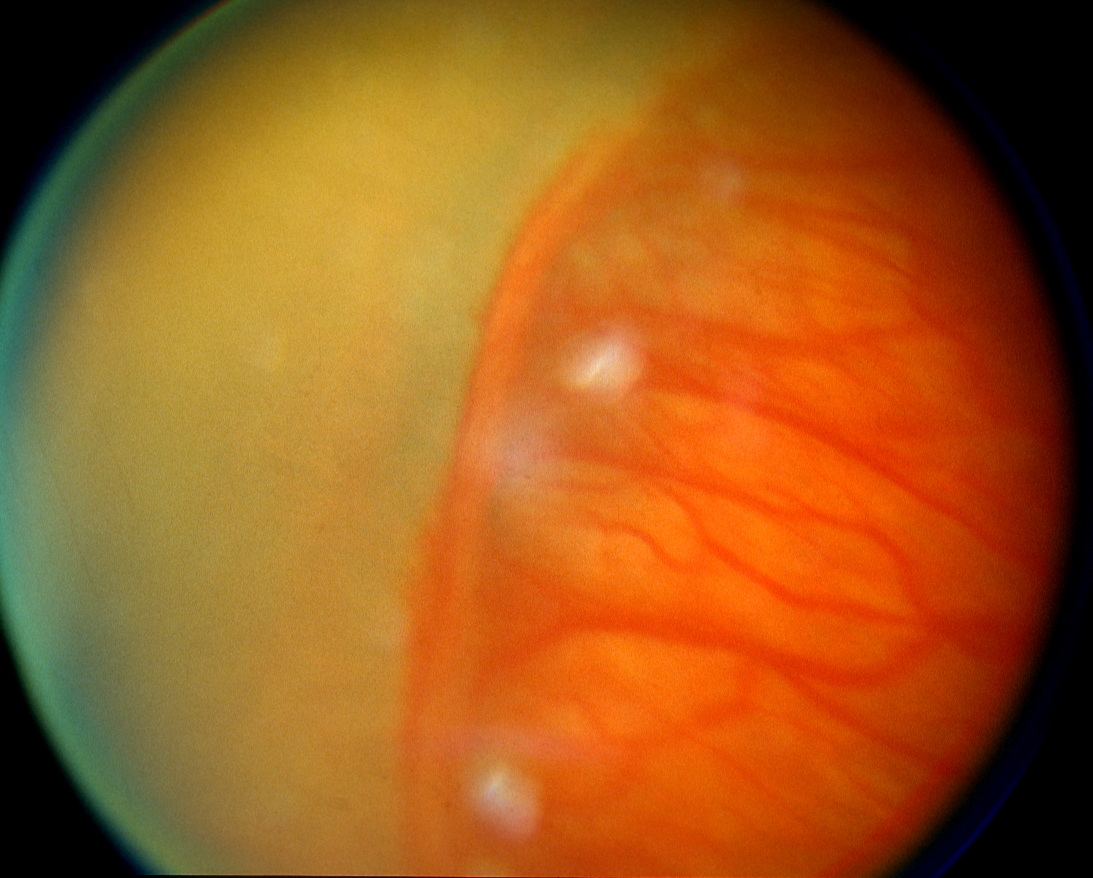
Image of a stage 2 demarcation line commonly seen in ROP
- Coats’ disease – abnormal development of temporal retinal vessels that is ten times more common in males, primarily affects only one eye and usually seen in patients younger than 8 years of age.

Fundus photo of the mass lipid exudation from leaky, telangiectatic vessels in Coat’s disease
- Persistent hyperplastic primary vitreous – usually unilateral and results from failure of regression of embryological vitreous and blood vessels and is often associated with a cataract or retrolental fibroplasia.
- Inflammation (i.e. ocular toxocariasis, congenital CMV) – any intraocular inflammatory process can cause leukocoria from an accumulation of inflammatory debris, especially if the vitreous is involved.
- Coloboma – results from failure of the developing eye to complete circumferential fusion of the developing nasal and temporal poles. Ocular colobomas occur inferiorly in the eye and can involve the optic nerve, retina, lens and/or iris. From a primary care perspective, an iris coloboma (an inferonasal defect in the iris) is most easily recognized as it is the most anterior. For such patients, referral to a pediatric ophthalmologist for a dilated eye exam is important to assess whether the coloboma has affected deeper structures within the eye.
- Familial exudative vitreoretinopathy (FEVR) – has features that overlap with ROP but with different patient characteristics (i.e. not premature) and disease time course. The hallmark features are peripheral zones of avascular retina that are prone to abnormal blood vessel formation, leakage and exudate formation, and vitreous traction that often results in retinal detachments.
- Retinal detachment – though rare in the pediatric population, there is increased prevalence of retinal detachments in patients with ROP, high myopia (near-sightedness), and other ophthalmologic problems like FEVR.
Diagnosis: The following modalities may be used by ophthalmic specialists to determine the cause of leukocoria:
- Direct ophthalmoscopy
- Slit lamp biomicroscopy and indirect ophthalmoscopy
- Retinal fundus photography
- Fluorescein Angiography
- Orbital/Head imaging often aids to narrow the differential diagnosis
- B-scan ultrasonography
- Optical coherence tomography (OCT)
- MRI of the head and orbits (CT scans are avoided in case of malignancy to avoid radiation exposure)
Management: Management of leukocoria varies and is dependent on the specific cause. Though retinoblastoma is the most feared cause of the leukocoria, many referrals for an asymmetric or abnormal red reflex turn out to be nothing. Nonetheless, a timely referral for a dilated eye exam is still vital. In the infant to toddler age range it is important to ask about a family history of retinoblastoma or congenital cataracts along with taking a careful birth and delivery history. In the case of a congenital cataract (which may be unilateral or bilateral), the timing of cataract surgery is amongst the most important factors in eventual visual outcomes. Unilateral cataracts are ideally removed at six weeks of ages and bilateral cataracts by eight to ten weeks. Missing this window can cause irreversible deprivational amblyopia, or permanent blindness in one or both eyes.
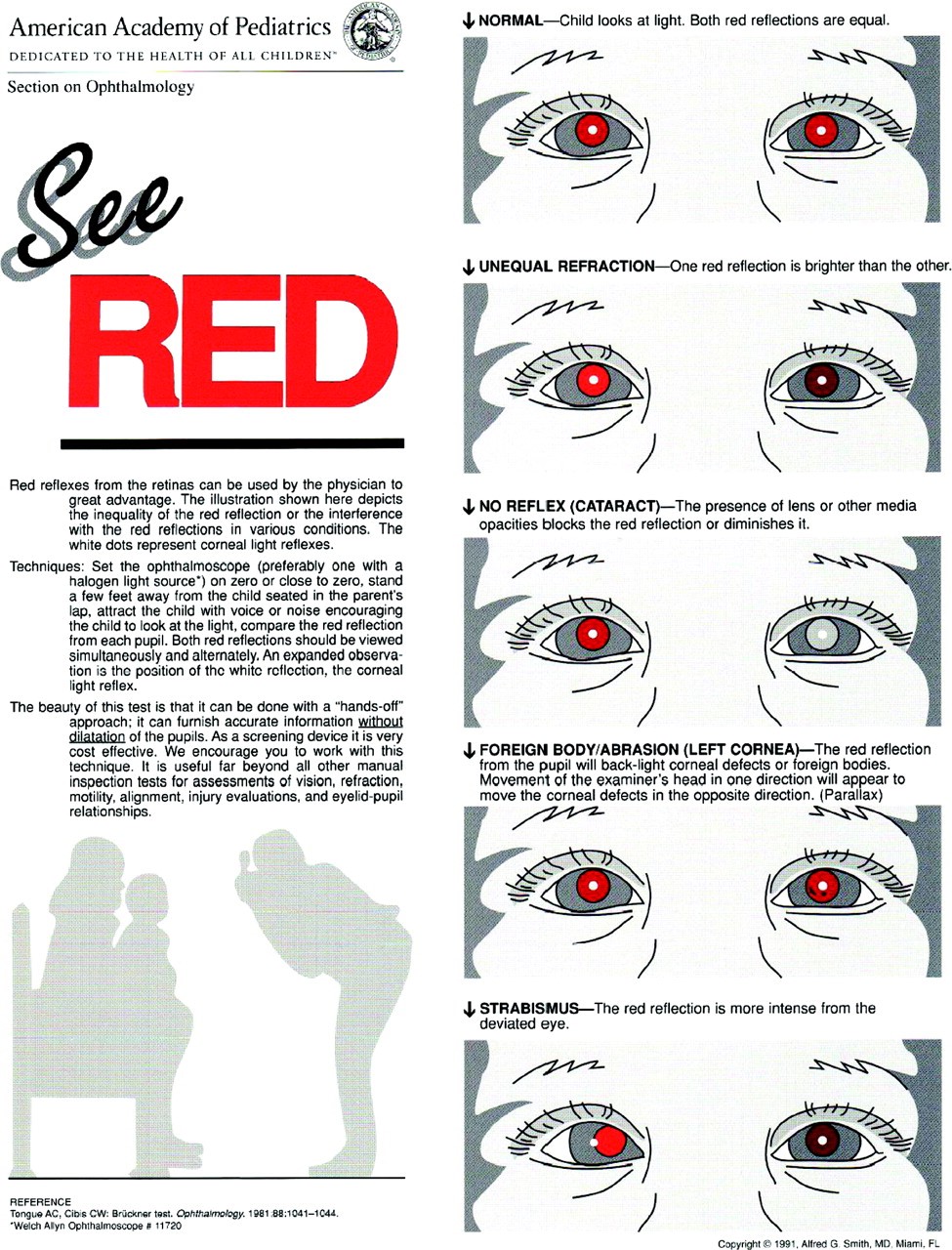
From: American Academy of Pediatrics. (2008). Red reflex examination in neonates, infants, and children. Pediatrics, 122(6), 1401-1404.
See Red handout from the American Academy of Pediatrics: http://pediatrics.aappublications.org/content/122/6/1401
References:
- Stagg, B., Ambati, BK. et al. (2014) Diagnostic Ophthalmology. Amirsys Publishing, Inc., Manitoba, Canada.
- Shields, J. A., Shields, C. L. (2008). Retinoblastoma: Introduction, Genetics, Clinical Features, Classification. In Intraocular Tumors: An Atlas and Textbook (pp. 293-318). Lippincott Williams & Wilkins, Philadelphia, PA.
- Shields, J. A., Shields, C. L. (2008). Retinoblastoma: Diagnostic Approaches. In Intraocular Tumors: An Atlas and Textbook (pp. 319-326). Lippincott Williams & Wilkins, Philadelphia, PA.
- Shields, J. A., Shields, C. L. (2008). Lesions That Can Simulate Retinoblastoma. In Intraocular Tumors: An Atlas and Textbook (pp. 353-366). Lippincott Williams & Wilkins, Philadelphia, PA.
- Balmer, A., & Munier, F. (1999). Leukokoria in a child: emergency and challenge. Klinische Monatsblatter Fur Augenheilkunde, 214(5), 332-335.
- Haider, S., Qureshi, W., & Ali, A. (2008). Leukocoria in children. Journal of pediatric ophthalmology and strabismus, 45(3), 179-180.
- American Academy of Pediatrics. (2008). Red reflex examination in neonates, infants, and children. Pediatrics, 122(6), 1401-1404.
Identifier: Moran_CORE_24126