
Scleritis
Home / Basic Ophthalmology Review / Conjunctiva / Sclera
Title: Scleritis
Author: Trey Winter, 1st Year Medical Student, University of Utah
Description: Scleritis is a disorder characterized by the inflammation of the sclera that can radiate to the cornea, episclera, and uveal tract. This inflammation can be destructive, painful, and potentially blinding. It is commonly associated with other systemic diseases such as rheumatoid arthritis.
Scleritis is divided into two main types, anterior scleritis and posterior scleritis. Anterior scleritis is further divided into three categories: diffuse anterior scleritis, nodular anterior scleritis, and necrotizing anterior scleritis.

Diffuse anterior scleritis- the most common, best prognosis.
Scleromalacia or corneal thinning from prior scleritis.

Necrotizing anterior scleritis- least common, most dangerous.

Nodular anterior scleritis- 2nd most common, often recurrent.
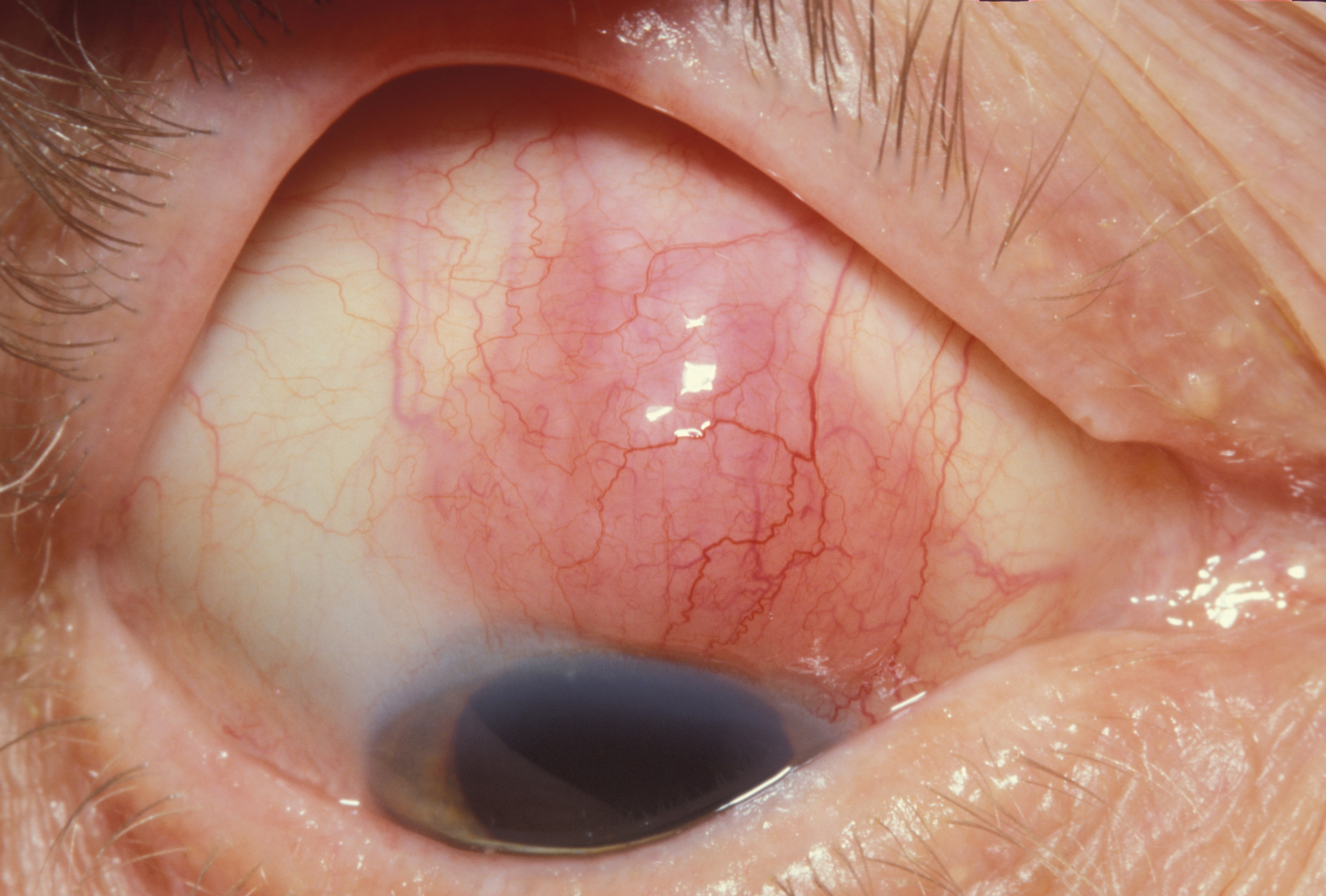
Presentation: Scleritis most commonly presents with severe, constant eye pain that worsens at night and in the morning. Movement of the eye is generally painful as the muscles controlling eye movement insert into the sensitized sclera. Patients with scleritis also present with ocular redness, headaches, photophobia, and watering of the eye.
The key sign of scleritis during ocular examination is an injection (an apparent increase in size and number of blood vessels on the sclera), associated with violaceous discoloration of the eye and tenderness to palpation. Although the injection can span multiple layers, involvement of the deep episcleral vascular plexus is what distinguishes scleritis from other, less severe conditions.
Diagnosis: It is important to note that the diagnosis of scleritis involves two aspects: the primary diagnosis of scleritis and the evaluation for a systemic disorder associated with scleritis.
Scleritis can be diagnosed and classified largely based on the information in the history and from the ophthalmologic exam. The ophthalmoscopy and slit-lamp examinations are used to detect deep scleral injection. Tenderness to palpation (done by gently pressing on the eyelid over the area of inflamed sclera) is highly specific to scleritis. A less common but occult form of scleritis known as “posterior scleritis” can present with a normal appearing external eye but instead present with choroidal and posterior scleral thickening on ultrasound.
The most important differential diagnosis is between scleritis and episcleritis. Episcleritis is an inflammation limited to the episclera (the layer superficial to the sclera) and is typically not emergent or vision-threatening. Both conditions present with similar symptoms including redness of the eye and pain. The phenylephrine test can be used to help distinguish these conditions by administering phenylephrine topically to the eye. In cases of episcleritis, the phenylephrine will blanch the eye due to vasoconstriction of the episcleral vessels. The deeper and larger inflamed vessels from sclerits will remain red after administration of the phenylephrine.
A large percentage of true scleritis cases have an underlying, associated systemic inflammatory condition. Here is a truncated list with a brief review of each disease:
- Rheumatoid Arthritis: an autoimmune condition that typically effects the patient’s joints. Include a physical exam of the joints for swelling, redness or deformity. Imaging of the joints or a blood test for rheumatoid factor or inflammatory factors are used.
- Granulomatosis with Polyangiitis (Wegener’s): a condition that causes inflammation of blood vessels. Classic symptoms of Wegener’s granulomatosis include sinus pain, cough, fever, blood in the urine, and occasionally hearing loss. It can be diagnosed with a blood test for anti-neutrophil cytoplasmic antibodies (ANCAs).
- Inflammatory bowel disease (IBD): presents with abdominal pains and cramps, abnormal and sometimes bloody stools, fever, and dehydration. On physical exam, carefully check for pain in the right lower quadrant of the abdomen.
- Shingles (Herpes Zoster Ophthalmicus): is a reaction to the varicella-zoster virus (VZV) that presents in and around the eye. Diagnosis is based on an eruption of vesicles along a single dermatome that typically last a few weeks.
- Other Conditions to Consider:
- Orbital inflammatory disease
- Lymphoma
- Sarcoidosis
- Lymphoproliferative disorder
- Orbital abscess
Complications: Scleritis can lead to permanent ocular complications in severe cases.
Complications from scleritis include:
- Scleromalacia (scleral thinning)
- Scleromalacia perforans (scleral rupture seen with necrotizing scleritis)
- Corneal changes
- Cataracts
- Glaucoma
- Retinal detachment
- Loss of vision
Management/Treatment: Treatment of scleritis usually begins with nonsteroidal anti-inflammatory drugs (NSAIDS), especially for diffuse anterior scleritis and nodular anterior scleritis. NSAIDS reduce the stiffness, swelling, and pain associated with scleritis. For necrotizing anterior scleritis and posterior scleritis, glucocorticoids or the combination of glucocorticoids and immunosuppressive agents are administered. In severe cases, patients need surgery to prevent rupture and retain vision.
Treatment is individualized based on the patient’s symptoms and the severity of the symptoms. As mentioned above, it is imperative not to forget a careful history and systemic work-up for any underlying, associated systemic inflammatory conditions.
Refrences:
- Benson WE. Posterior scleritis. Survey of Ophthalmology 1988; 5:297.
- Fong LP, Sainz de la Maza M, Rice BA, et al. Immunopathology of scleritis. Ophthalmology 1991; 98:472.
- Jabs DA, Mudun A, Dunn JP, Marsh MJ. Episcleritis and scleritis: clinical features and treatment results. Am J Ophthalmol 2000; 130:469.
- McCluskey PJ, Watson PG, Lightman S, et al. Posterior scleritis: clinical features, systemic associations, and outcome in a large series of patients. Ophthalmology 1999; 106:2380.
- Okhravi N, Odufuwa B, McCluskey P, Lightman S. Scleritis. Survey of Ophthalmology 2005; 50:351-363.
- Tuft SJ, Watson PG. Progression of scleral disease. Ophthalmology 1991; 98:467.
- Watson PG, Hayreh SS. Scleritis and episcleritis. British Journal of Ophthalmology 1976; 60:163-191.
- Albini TA, Rao NA, Smith RE. The Diagnosis and Management of Anterior Scleritis. International Ophthalmology Clinics 2005; 45:191-204.
Identifier: Moran_CORE_24943
Copyright statement: Copyright 2018. Please see terms of use page for more information.