
Ocular Side-Effects of Corticosteroids
Home / Basic Ophthalmology Review / Ocular Adverse Effects of Systemic Medications
Title: Ocular Side-Effects of Corticosteroids
Author(s): Sahil Aggarwal, MS4, University of California, Irvine School of Medicine; Brian Ta, MS4, University of Utah School of Medicine
Photographer: James Gilman, CRA, FOPS, Moran Eye Center Date: 07/2018
Keywords/Main Subjects:
CORE Category: Medical Student Education Outline > II. Anatomical Approach to Eye Disease > Ocular Adverse Effects of Systemic Medications > 1. Oral/topical/injected/inhaled Steroids
BACKGROUND
From local skin reactions to systemic autoimmune disorders, corticosteroids are an essential treatment modality for a wide spectrum of disease processes. However, as efficacious as they are therapeutically, they are heavily polluted with side effects. Patients chronically taking steroids often exhibit signs of metabolic syndrome, with elevated blood sugar, hypertension, and rapid weight gain. Additional adverse effects include easy bruising, osteoporosis, and emotional disturbances.1
In ophthalmology, steroids are predominantly used for treating inflammatory, autoimmune, and infectious diseases. They are often the first-line therapy in otherwise blinding conditions such as uveitis (inflammation of the uvea, or the pigmented layer of the eye including the iris, ciliary body and choroid) and giant cell arteritis.
There are several ocular side effects that are important to consider when prescribing steroids.2 It is important to note that all methods of steroid administration, including oral, topical, and inhalation, increase the risk for ocular side effects.3 Because of these risks, steroids must be used with caution and only when necessary.
MECHANISM OF ACTION
Corticosteroids exert their efficacy by altering the way genes are expressed throughout the body. In particular, gene products that are involved in inflammatory pathways are down-regulated, reducing the activity of inflammatory cells.4 Specific cascades affected by steroids include cytokine production and the arachidonic acid pathway, reducing the body’s ability to regulate inflammation.4 While inhibition of inflammatory cascades is vital to steroids’ treatment efficacy, the down-regulation of the immune system can lead to increased risk of infection.
OCULAR SIDE EFFECTS
There are four important ocular side effects of corticosteroids: steroid-induced glaucoma, cataract formation, delayed wound healing, and increased susceptibility to infection.
Glaucoma

Figure 1: A fundus photo of the optic nerve showing increased cupping, a risk factor for glaucoma.
Glaucoma is a condition in which there is damage to the optic nerve, often related to elevated intraocular pressure (IOP). The result of this damage is a progressive, permanent vision loss. Steroid use can cause an increase in IOP by increasing the expression of ocular extracellular matrix proteins, thus increasing resistance to the outflow of aqueous from the eye.5 The risk of steroid-induced glaucoma depends on the duration of use and potency of the steroids themselves as well as the individual’s baseline risk for glaucoma.6-8 The risks factors that have been identified to place someone at risk for a steroid-induced increase in IOP include: pre-existing primary open angle glaucoma, a history of increased IOP with previous steroid administration, a diagnosis of Type 1 diabetes, or those who are very young or very old.9 Patients who are taking steroids long-term should be regularly evaluated by ophthalmology for IOP changes, and consideration for non-steroid medications should always be made.
Cataracts
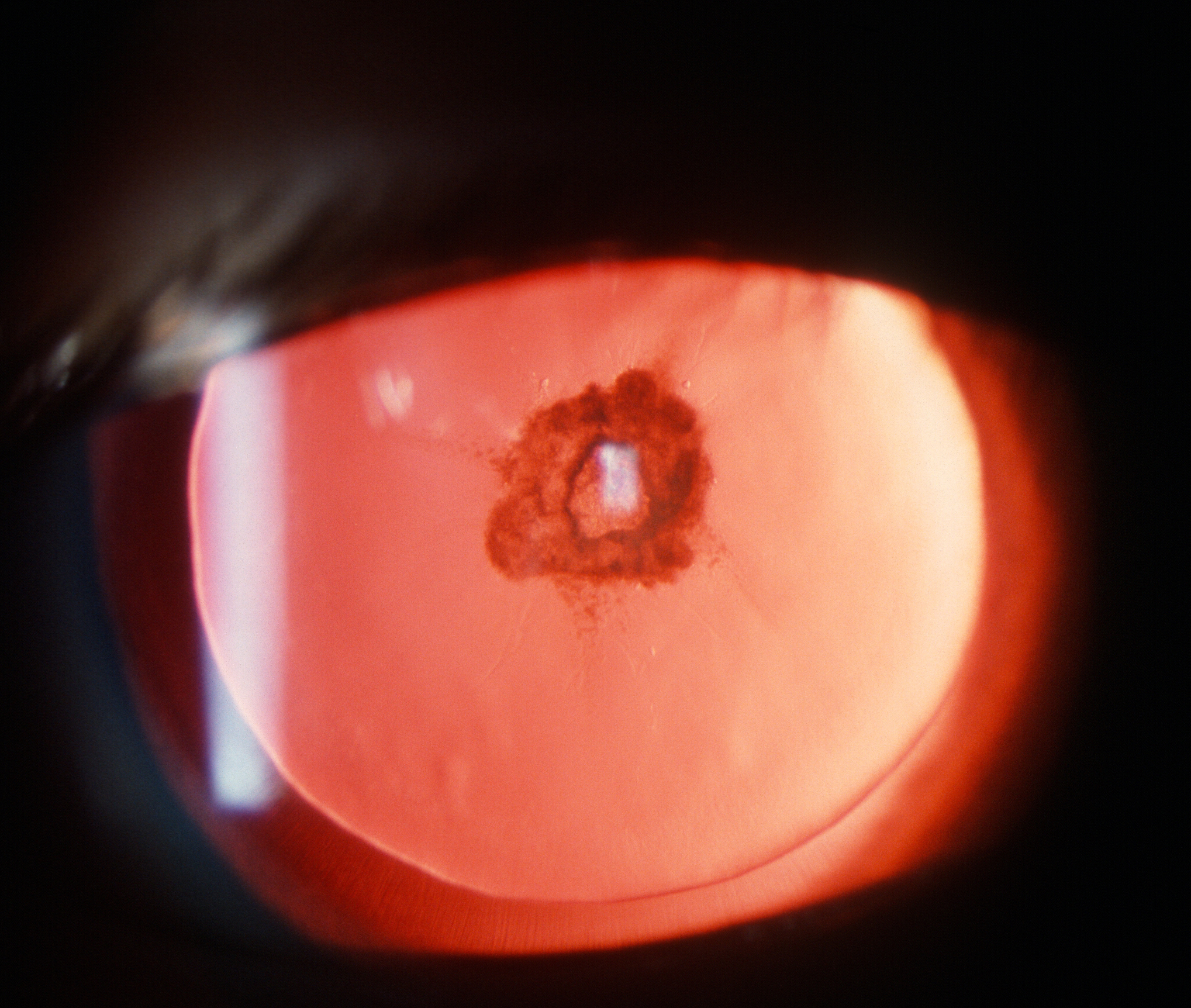
Figure 2. Example of a posterior subcapsular cataract, the type of cataract that often forms from chronic steroid use. Photographer: James Gilman, CRA, FOPS, Moran Eye Center11
Cataracts are a common finding in aging adults and are safely removed and replaced with an artificial lens during cataract surgery. Long-term steroid use is associated with an accelerated development of cataracts. While the mechanism of cataract development in this setting is not well understood, it is thought to involve steroid-induced changes in gene transcription within lens epithelial cells.10 Classically, the type of cataract associated with steroid use is called a posterior subcapsular cataract, which forms in the back of the lens (Figure 1).11 Patients on steroids who are experiencing reduced vision should be evaluated by an ophthalmologist.
Delayed Wound Healing and Risk of Infection

Figure 3: Fluorescein staining of a dendritic ulcer, pathognomonic for herpetic keratitis. This is a type of corneal ulcer where steroids are absolutely contraindicated due to the risk of worsening the infection.
Steroids are often used in conjunction with topical antibiotics in ocular infections such as corneal ulcers. However, previous research has identified that steroids inhibit growth factors critical in wound healing.12 Similarly, without co-treatment with antibiotics, local ocular infections that are treated with steroids may become worse, especially viral infections such as herpetic keratitis.12 While local steroid therapy is valuable in infections of the eye, owing to their ability to reduce inflammation and scarring, these benefits must be weighed against the risk of recurrent infection and poor wound healing and require the close monitoring of an eye specialist.
CONCLUSION
Corticosteroids are vitally important in treating several systemic and local inflammatory or autoimmune conditions. While therapy is associated with side effects, including steroid-induced glaucoma, cataracts, poor wound healing, and progressing infections, these effects can be mitigated with attentive monitoring.13 Non-ophthalmologists should strongly consider referring any patient on prolonged systemic steroids to an eye-care specialist for monitoring for glaucoma and cataracts. The decision to prescribe topical steroids can be complex and should involve an ophthalmologist.
REFERENCES
1. Buchman AL. Side effects of corticosteroid therapy. J Clin Gastroenterol 2001;33:289–94.
2. Renfro L, Snow JS. Ocular effects of topical and systemic steroids. Dermatol Clin
1992;10:505–12.
3. Daniel BS, Orchard D. Ocular side-effects of topical corticosteroids: what a dermatologist
needs to know. Australas J Dermatol 2015;56:164–9.
4. Comstock TL, DeCory HH. Advances in Corticosteroid Therapy for Ocular Inflammation:
Loteprednol Etabonate. Int J Inflam 2012;2012.
5. Phulke S, Kaushik S, Kaur S, et al. Steroid-induced Glaucoma: An Avoidable Irreversible
Blindness. J Curr Glaucoma Pract 2017;11:67–72.
6. Francois J. Cortisone et tension oculaire. Ann D’Oculist 1954; 187: 805.
7. Cantrill HL, Palmberg, Zink HA, Waltman SR, Podos SM, Becker B. Comparison of in
vitro potency of corticosteroids with ability to raise intraocular pressure. Am J
Ophthalmol 1975; 79: 1012–1017.
8. Francois J. Corticosteroid glaucoma. Ann Ophthalmol 1977; 9: 1075–1080.
9. Goñi FJ, Stalmans I, Denis P, et al. Elevated Intraocular Pressure After Intravitreal Steroid
Injection in Diabetic Macular Edema: Monitoring and Management. Ophthalmol Ther
2016;5:47–61.
10. James ER. The etiology of steroid cataract. J Ocul Pharmacol Ther 2007;23:403–20.
11. Moran CORE | Cataracts. http://morancore.utah.edu/medical-student-education-
outline/cataracts/ (accessed 28 Jul 2018).
12. Srinivasan M, Mascarenhas J, Rajaraman R, et al. The Steroids for Corneal Ulcers Trial.
Arch Ophthalmol 2012;130.
13. Abelson MB, Butrus S. Corticosteroids in ophthalmic practice. Chapter 23. In: Albert DM et
al., eds. Albert & Jakobiec’s Principles and Practice of Ophthalmology, 3rd ed.
Philadelphia: Saunders Elsevier; 2008.